Department of Colorectal Surgery, The Sixth Affiliated Hospital (The Gastrointestinal & Anal Hospital) of Sun Yat-sen University, Guangzhou, China and Department of Oncology, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Gastroenterol Rep (Oxf). 2014 Feb;2(1):37-43. doi: 10.1093/gastro/got040. Epub 2014 Jan 21.
With the increased usage of neoadjuvant chemoradiotherapy, improved surgical technique and stapling devices, sphincter-preserving resection has become more frequent for patients with rectal cancer. However, as for locally advanced ultra-low rectal cancer, sphincter-preservation is still facing an enormous challenge.
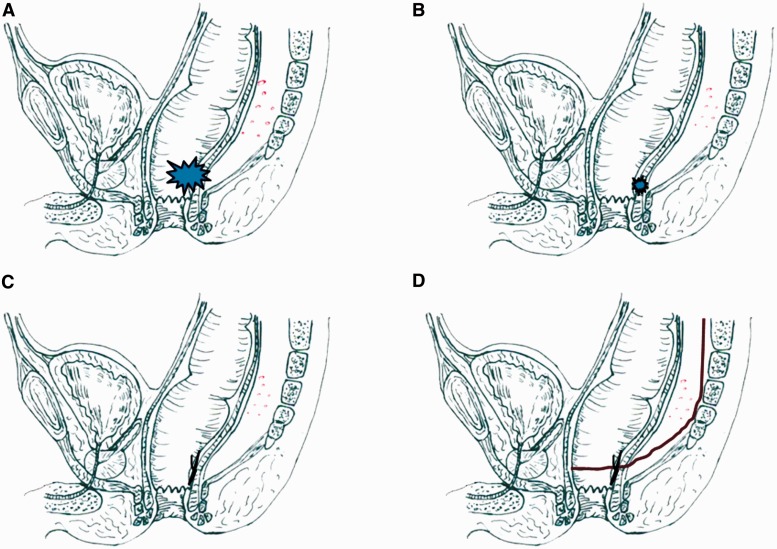
To introduce an NLT strategy of sphincter-preservation-neoadjuvant therapy (NT) followed by local excision (LE) and two-stage total mesorectal excision (TME)-into the treatment of locally advanced ultra-low rectal cancer (lesions with anal sphincter invasion).
From October 2010 to October 2011, nine patients with locally advanced rectal cancer located less than 3 cm from the anal verge were treated by the NLT strategy. All patients had shown good clinical response to NT. The LE procedure was carried transanally 6-8 weeks after completion of the NT. TME was performed to dissect mesorectal lymph nodes 4-6 weeks after LE.
Of the nine patients, the lesion was assessed as T2 in two, T3 in five, and T4 in two before NT, and lymph node metastasis was detected in five patients. The median distance from the tumor to the anal verge was 2.5 cm (range: 1-3 cm). The median follow-up was 27 months (range: 24-34 months). No distant metastasis was detected. Only one patient (11.1%) developed local recurrence at 12 months post-operatively and then underwent abdomino-perineal resection. The remaining eight patients had preserved long-term continence and the median Wexner score at two years post-operation was 4 (range: 2-6).
The new NLT strategy can achieve sphincter-preservation in some patients with ultra-low rectal cancer, with favorable oncological outcome and preservation of normal anal sphincter function.
随着新辅助放化疗的应用增加、手术技术的改进以及吻合器的应用,保肛手术在直肠癌患者中的应用越来越频繁。然而,对于局部进展期超低位直肠癌,保肛仍然面临巨大挑战。
介绍一种新的低位直肠癌保肛策略——新辅助治疗(NT)联合局部切除(LE)和两阶段全直肠系膜切除术(TME),用于治疗局部进展期超低位直肠癌(侵犯肛门括约肌的病变)。
2010 年 10 月至 2011 年 10 月,采用新辅助治疗策略治疗 9 例距离肛缘小于 3cm 的局部进展期直肠癌患者。所有患者对 NT 均有良好的临床反应。NT 完成后 6-8 周内行经肛门 LE 手术。LE 术后 4-6 周行 TME 以解剖直肠系膜淋巴结。
9 例患者中,NT 前肿瘤评估为 T2 2 例,T3 5 例,T4 2 例,5 例患者检测到淋巴结转移。肿瘤距肛缘的中位距离为 2.5cm(范围:1-3cm)。中位随访时间为 27 个月(范围:24-34 个月)。无远处转移。术后 12 个月仅 1 例患者(11.1%)发生局部复发,随后行腹会阴联合切除术。其余 8 例患者长期保肛,术后 2 年中位 Wexner 评分 4 分(范围:2-6 分)。
新的 NT 策略可使部分超低位直肠癌患者保肛,且具有良好的肿瘤学结果和正常肛门括约肌功能的保留。