Population Council, Ralph Bunche Rd,, PO Box 17643-00500, Nairobi, Kenya.
Int J Equity Health. 2014 Apr 29;13:33. doi: 10.1186/1475-9276-13-33.
Developing countries face challenges in financing healthcare; often the poor do not receive the most basic services. The past decade has seen a sharp increase in the number of voucher programs, which target output-based subsidies for specific services to poor and underserved groups. The dearth of literature that examines lessons learned risks the wheel being endlessly reinvented. This paper examines commonalities and differences in voucher design and implementation, highlighting lessons learned for the design of new voucher programmes.
The methodology comprised: discussion among key experts to develop inclusion/exclusion criteria; up-dating the literature database used by the DFID systematic review of voucher programs; and networking with key contacts to identify new programs and obtain additional program documents. We identified 40 programs for review and extracted a dataset of more than 120 program characteristics for detailed analysis.
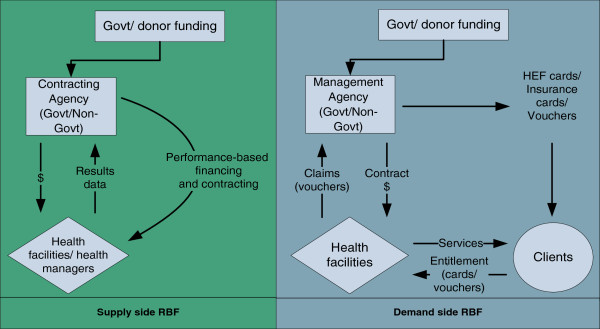
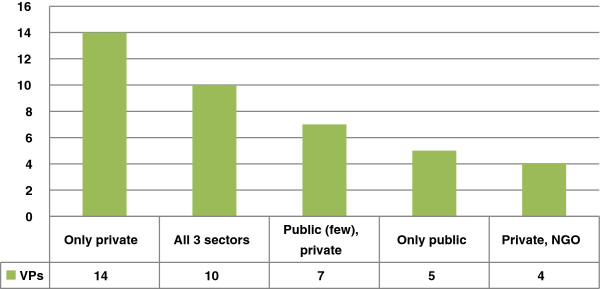
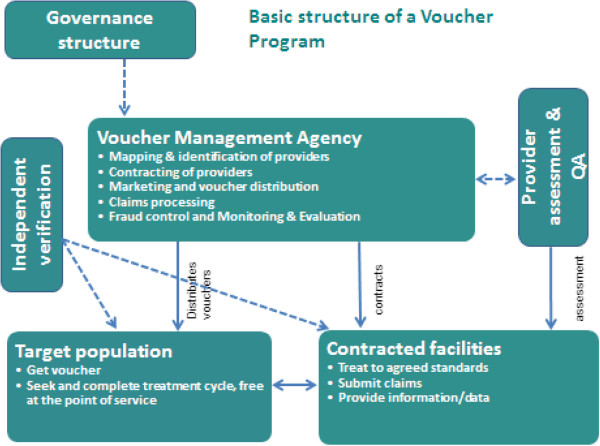
All programs aimed to increase utilisation of healthcare, particularly maternal health services, overwhelmingly among low-income populations. The majority contract(ed) private providers, or public and private providers, and all facilitate(d) access to services that are well defined, time-limited and reflect the country's stated health priorities. All voucher programs incorporate a governing body, management agency, contracted providers and target population, and all share the same incentive structure: the transfer of subsidies from consumers to service providers, resulting in a strong effect on both consumer and provider behaviour. Vouchers deliver subsidies to individuals, who in the absence of the subsidy would likely not have sought care, and in all programs a positive behavioural response is observed, with providers investing voucher revenue to attract more clients. A large majority of programs studied used targeting mechanisms.
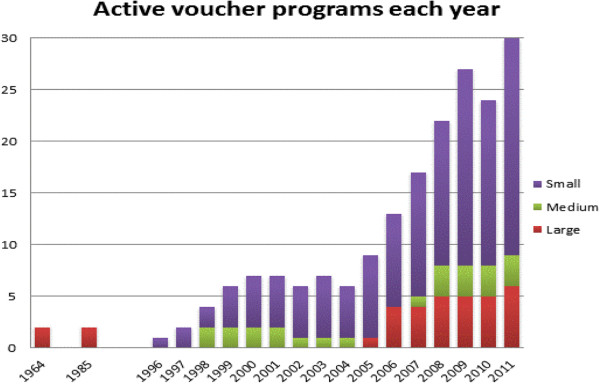
While many programs remain too small to address national-level need among the poor, large programs are being developed at a rate of one every two years, with further programs in the pipeline. The importance of addressing inequalities in access to basic services is recognized as an important component in the drive to achieve universal health coverage; vouchers are increasingly acknowledged as a promising targeting mechanism in this context, particularly where social health insurance is not yet feasible.
发展中国家在医疗保健融资方面面临挑战;通常情况下,穷人无法获得最基本的服务。在过去的十年中,针对贫困和服务不足群体的特定服务的基于产出的补贴的代金券计划数量急剧增加。由于缺乏审查所吸取经验教训的文献,这有可能导致无休止地重新发明轮子。本文研究了代金券设计和实施的异同之处,重点介绍了为新代金券计划设计提供的经验教训。
该方法包括:关键专家讨论以制定纳入/排除标准;更新英国国际发展部代金券计划系统评价使用的文献数据库;与主要联系人建立联系以确定新计划并获取额外的计划文件。我们确定了 40 个计划进行审查,并提取了一个包含 120 多个计划特征的数据集进行详细分析。
所有计划都旨在增加医疗保健的利用,特别是孕产妇保健服务,绝大多数都是针对低收入人群。大多数计划与私营提供者或公私提供者签订合同,并为明确规定的、有时限的、反映国家既定卫生重点的服务提供便利。所有代金券计划都包含一个管理机构、管理机构、签约提供者和目标人群,并且都具有相同的激励结构:从消费者向服务提供者转移补贴,从而对消费者和提供者的行为都产生强烈影响。代金券将补贴提供给个人,如果没有补贴,他们可能不会寻求医疗服务,并且在所有计划中都观察到了积极的行为反应,提供者投资代金券收入以吸引更多客户。研究中的大多数计划都使用了目标定位机制。
虽然许多计划仍然太小,无法满足穷人的国家一级需求,但大型计划正在以每两年一个的速度开发,并且还有更多的计划正在筹备中。解决获得基本服务方面的不平等问题被认为是实现全民健康覆盖的重要组成部分;代金券在这种情况下越来越被认为是一种有前途的目标定位机制,特别是在社会医疗保险还不可行的情况下。