Center for Cardiovascular Health Services Research, Institute for Clinical Research and Health Policy Studies, Tufts Medical Center and Tufts University School of Medicine, Boston, Massachusetts.
Division of Cardiology and the CardioVascular Center, Tufts Medical Center and Tufts University School of Medicine, Boston, Massachusetts.
Am J Cardiol. 2014 May 15;113(10):1599-605. doi: 10.1016/j.amjcard.2014.02.010. Epub 2014 Mar 1.
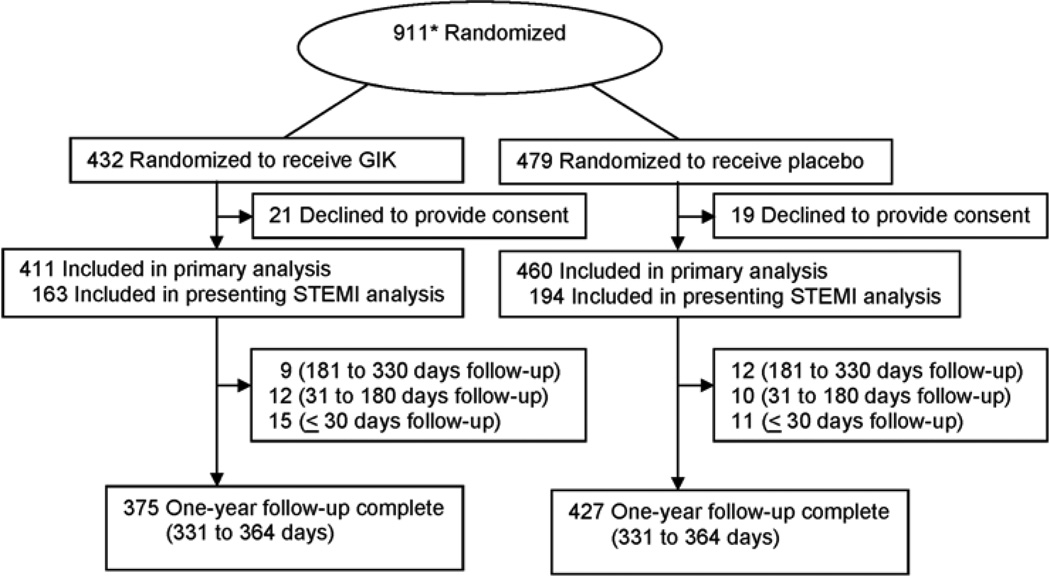
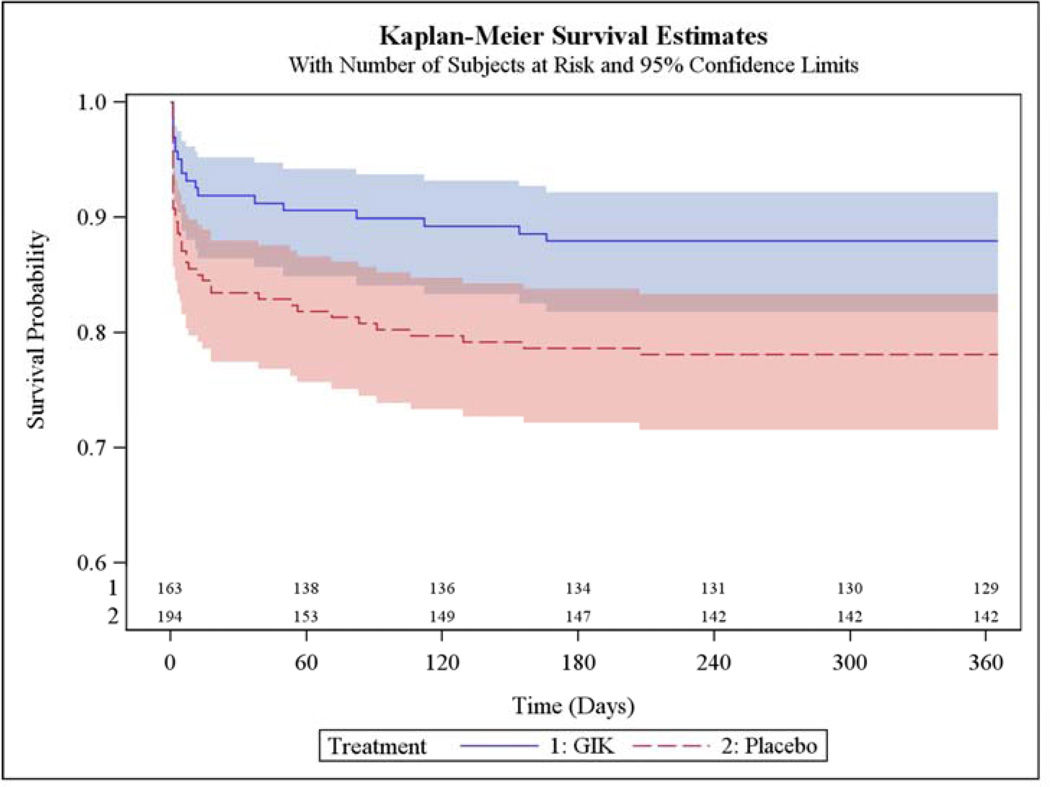
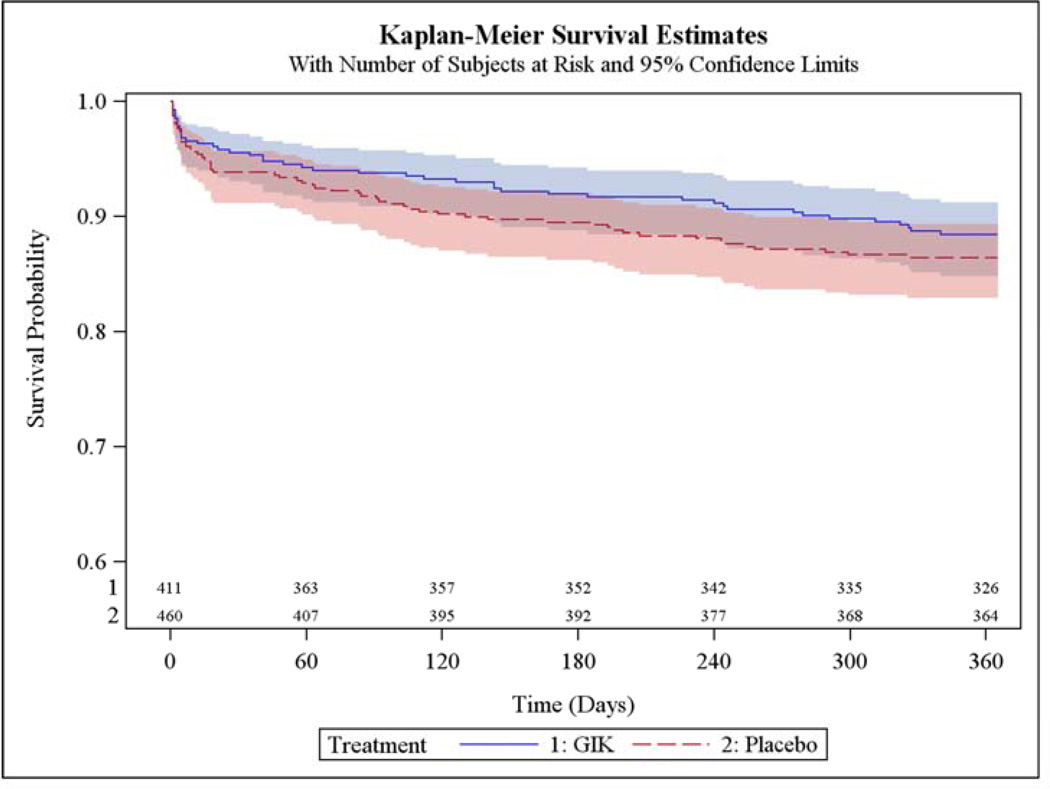
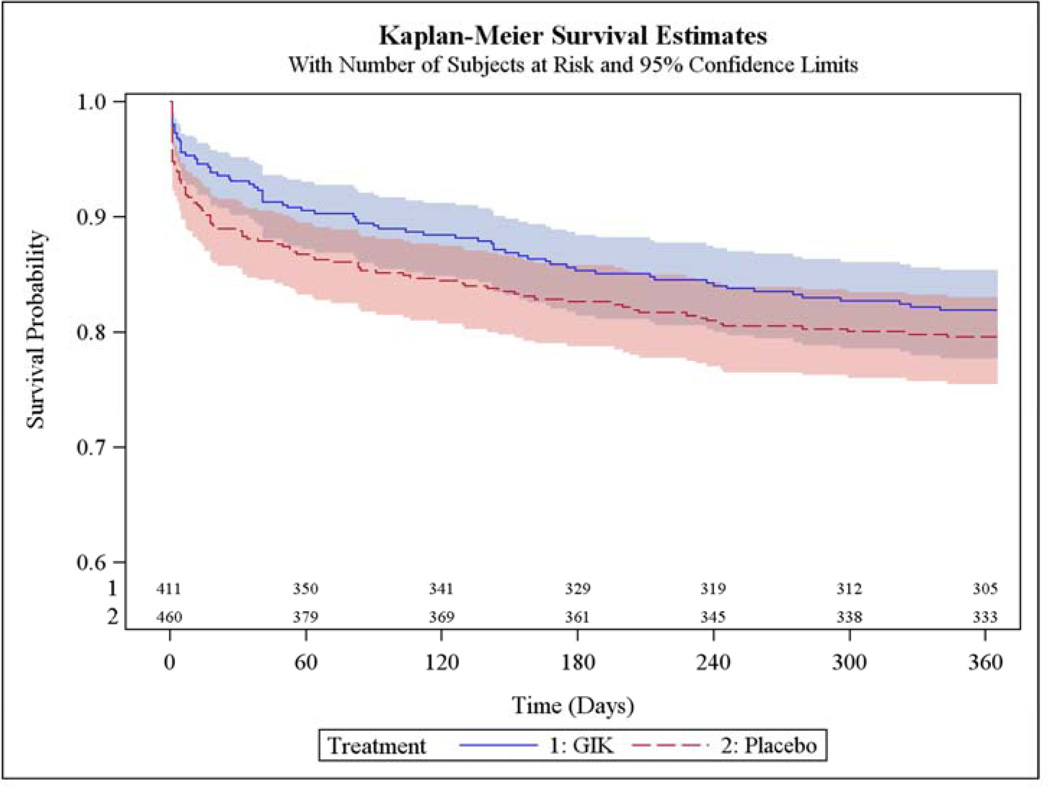
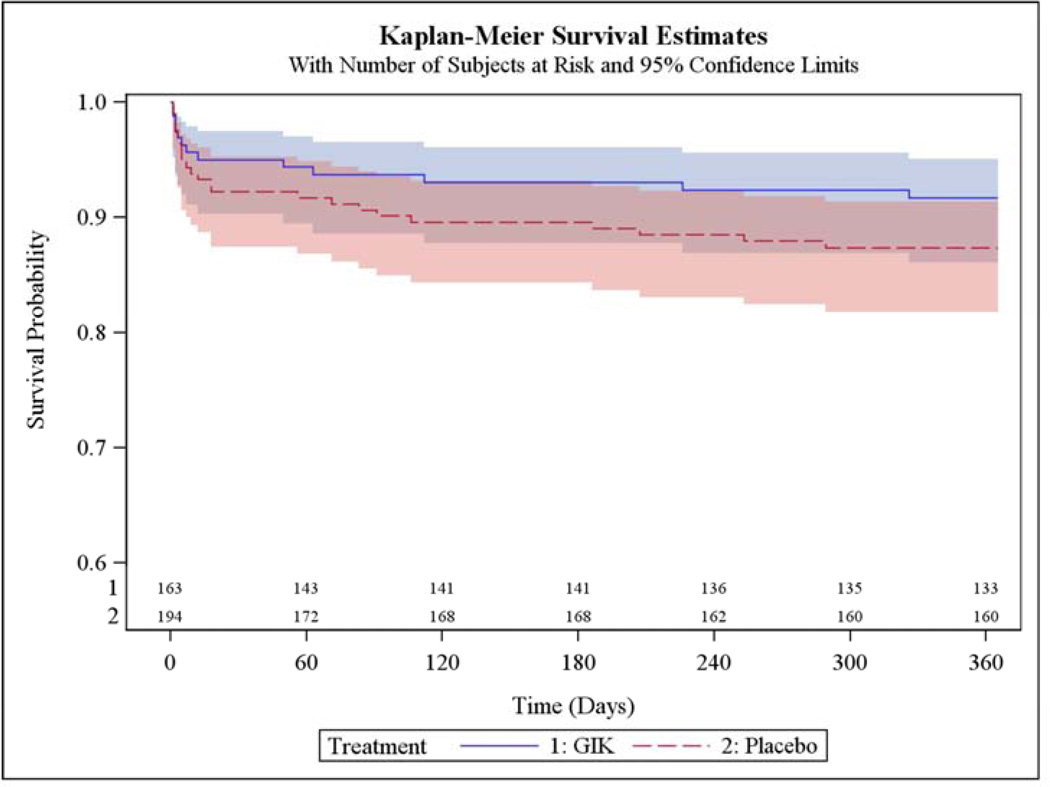
The Immediate Myocardial Metabolic Enhancement During Initial Assessment and Treatment in Emergency care Trial of very early intravenous glucose-insulin-potassium (GIK) for acute coronary syndromes (ACS) in out-of-hospital emergency medical service (EMS) settings showed 80% reduction in infarct size at 30 days, suggesting potential longer-term benefits. Here we report 1-year outcomes. Prespecified 1-year end points of this randomized, placebo-controlled, double-blind, effectiveness trial included all-cause mortality and composites including cardiac arrest, mortality, or hospitalization for heart failure (HF). Of 871 participants randomized to GIK versus placebo, death occurred within 1 year in 11.6% versus 13.5%, respectively (unadjusted hazard ratio [HR] 0.83, 95% confidence interval [CI] 0.57 to 1.23, p = 0.36). The composite of cardiac arrest or 1-year mortality was 12.8% versus 17.0% (HR 0.71, 95% CI 0.50 to 1.02, p = 0.06). The composite of hospitalization for HF or mortality within 1 year was 17.2% versus 17.2% (HR 0.98, 95% CI 0.70 to 1.37, p = 0.92). The composite of mortality, cardiac arrest, or HF hospitalization within 1 year was 18.1% versus 20.4% (HR 0.85, 95% CI 0.62 to 1.16, p = 0.30). In patients presenting with suspected ST elevation myocardial infarction, HRs for 1-year mortality and the 3 composites were, respectively, 0.65 (95% CI 0.33 to 1.27, p = 0.21), 0.52 (95% CI 0.30 to 0.92, p = 0.03), 0.63 (95% CI 0.35 to 1.16, p = 0.14), and 0.51 (95% CI 0.30 to 0.87, p = 0.01). In patients with suspected acute coronary syndromes, serious end points generally were lower with GIK than placebo, but the differences were not statistically significant. However, in those with ST elevation myocardial infarction, the composites of cardiac arrest or 1-year mortality, and of cardiac arrest, mortality, or HF hospitalization within 1 year, were significantly reduced.
在院外急救医疗服务(EMS)环境中,极早期静脉内葡萄糖-胰岛素-钾(GIK)治疗对急性冠脉综合征(ACS)的初始评估和治疗期间的即刻心肌代谢增强试验显示,30 天时梗死面积减少 80%,提示可能有更长时间的益处。在此,我们报告了 1 年的结果。这项随机、安慰剂对照、双盲、有效性试验的预先指定的 1 年终点包括全因死亡率和包括心搏骤停、死亡率或心力衰竭(HF)住院在内的复合终点。在随机分配至 GIK 组和安慰剂组的 871 名患者中,分别有 11.6%和 13.5%的患者在 1 年内死亡(未调整的危险比[HR]0.83,95%置信区间[CI]0.57 至 1.23,p=0.36)。心搏骤停或 1 年死亡率的复合终点为 12.8%和 17.0%(HR 0.71,95%CI 0.50 至 1.02,p=0.06)。1 年内 HF 或死亡率的复合终点为 17.2%和 17.2%(HR 0.98,95%CI 0.70 至 1.37,p=0.92)。1 年内死亡率、心搏骤停或 HF 住院的复合终点为 18.1%和 20.4%(HR 0.85,95%CI 0.62 至 1.16,p=0.30)。在疑似 ST 段抬高型心肌梗死的患者中,1 年死亡率和 3 项复合终点的 HR 分别为 0.65(95%CI 0.33 至 1.27,p=0.21)、0.52(95%CI 0.30 至 0.92,p=0.03)、0.63(95%CI 0.35 至 1.16,p=0.14)和 0.51(95%CI 0.30 至 0.87,p=0.01)。在疑似急性冠脉综合征的患者中,GIK 组的严重终点通常低于安慰剂组,但差异无统计学意义。然而,在 ST 段抬高型心肌梗死患者中,心搏骤停或 1 年死亡率的复合终点,以及心搏骤停、死亡率或 1 年内 HF 住院的复合终点显著降低。