Bosteels Jan, Weyers Steven, Mol Ben W J, D'Hooghe Thomas
Department of Obstetrics and Gynaecology, Imeldahospitaal, Imeldalaan 9, 2820 Bonheiden, Belgium ; CEBAM, Centre for Evidence-based Medicine, the Belgian Branch of the Dutch Cochrane Centre, ACHG, Kapucijnenvoer 33, blok J bus 7001, 3000 Leuven, Belgium.
Universitaire Vrouwenkliniek, University Hospital Gent, De Pintelaan 185, 9000 Gent, Belgium.
Gynecol Surg. 2014;11(2):113-127. doi: 10.1007/s10397-014-0832-x. Epub 2014 Mar 14.
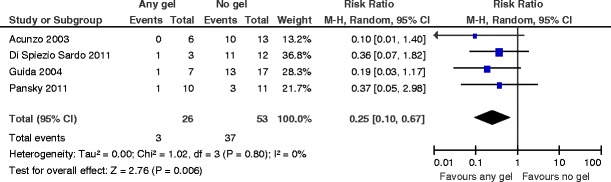
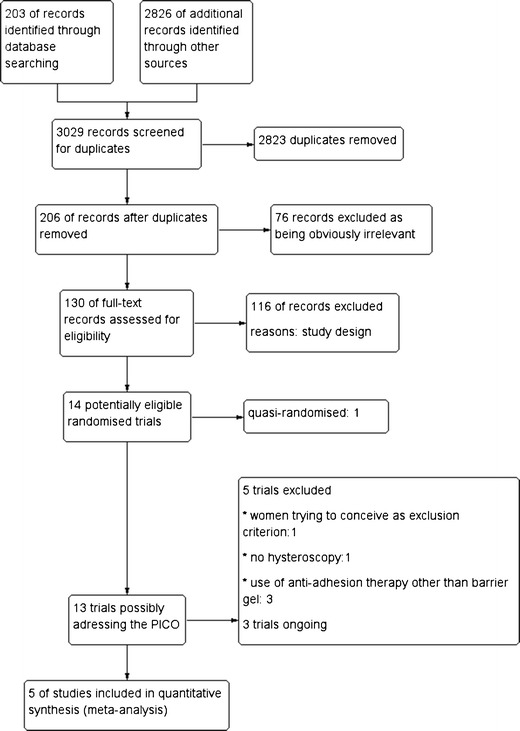
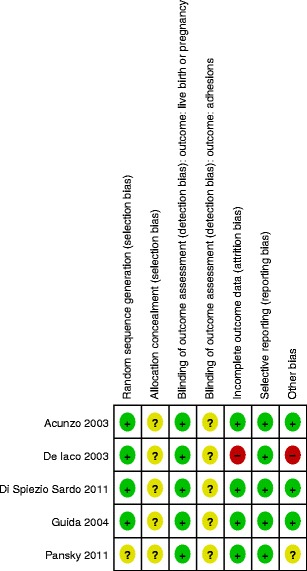
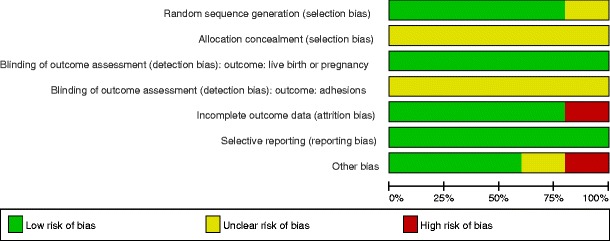
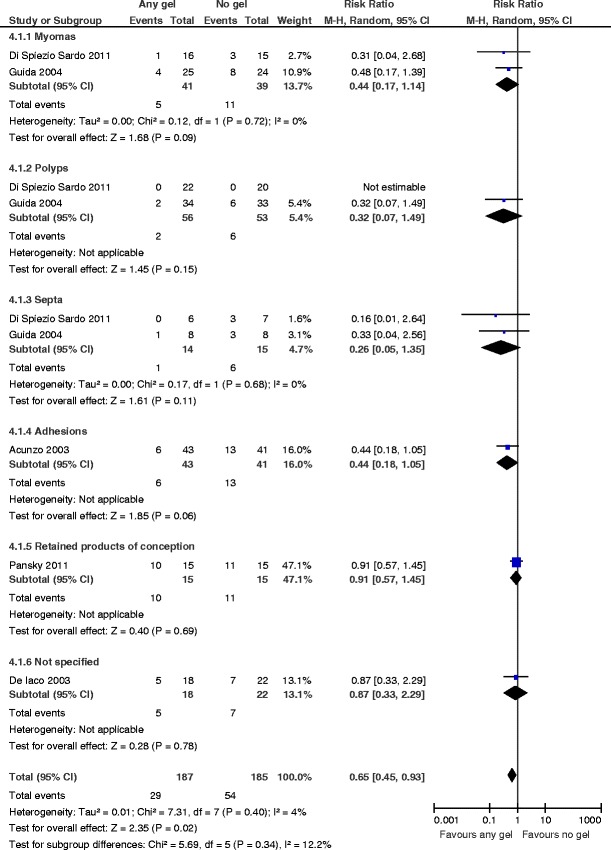
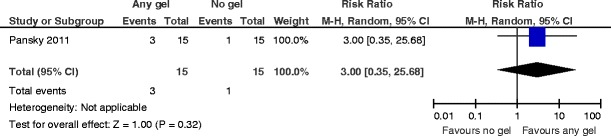
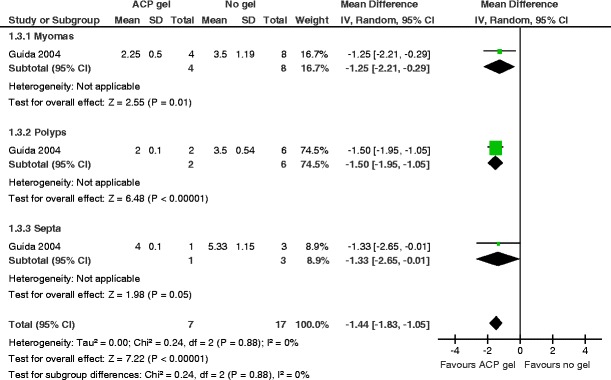
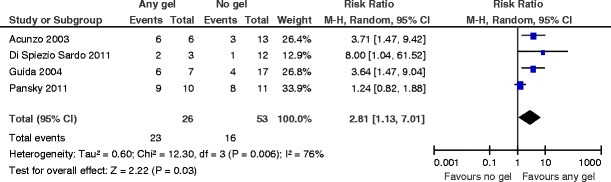
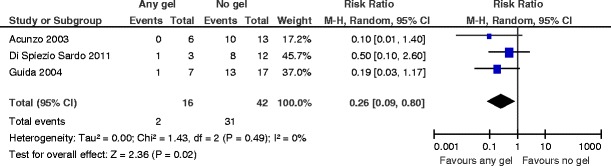
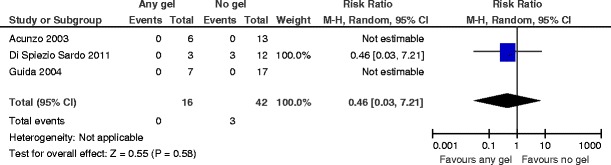
The aim of this study was to assess the effects of any anti-adhesion barrier gel used after operative hysteroscopy for treating infertility associated with uterine cavity abnormalities. Gynecologists might use any barrier gel following operative hysteroscopy in infertile women for decreasing de novo adhesion formation; the use of any barrier gel is associated with less severe de novo adhesions and lower mean adhesion scores. Nevertheless, infertile women should be counseled that there is at the present no evidence for higher live birth or pregnancy rates. There is a lack of data for the outcome miscarriage. Preclinical studies suggest that the use of biodegradable surgical barriers may decrease postsurgical adhesion formation. Observational studies in the human report conflicting results. We searched the Cochrane Menstrual Disorders and Subfertility Specialized Register (10 April 2013), the Cochrane Central Register of Controlled Trials ( 2013, Issue 1), MEDLINE (1950 to 4 April 2013), EMBASE (1974 to 4 April 2013), and other electronic databases of trials including trial registers, sources of unpublished literature, and reference lists. We handsearched the (from 1 January 1992 to 13 April 2013); we also contacted experts in the field. We included the randomized comparisons between any anti-adhesion barrier gel versus another barrier gel, placebo, or no adjunctive therapy following operative hysteroscopy. Primary outcomes were live birth rates and de novo adhesion formation at second-look hysteroscopy. Secondary outcomes were pregnancy and miscarriage rates, mean adhesion scores, and severity of adhesions at second-look hysteroscopy. Two authors independently assessed eligible studies for inclusion and risk of bias, and extracted data. We contacted primary study authors for additional information or other clarification. Five trials met the inclusion criteria. There is no evidence for an effect favoring the use of any barrier gel following operative hysteroscopy for the key outcomes of live birth or clinical pregnancy (risk ratio (RR) 3.0, 95 % confidence interval (CI) 0.35 to 26, = 0.32, one study, 30 women, very low quality evidence); there were no data on the outcome miscarriage. The use of any gel following operative hysteroscopy decreases the incidence of de novo adhesions at second-look hysteroscopy at 1 to 3 months (RR 0.65, 95 % CI 0.45 to 0.93, = 0.02, five studies, 372 women, very low quality evidence). The number needed to treat to benefit is 9 (95 % CI 5 to 33). The use of auto-cross-linked hyaluronic acid gel in women undergoing operative hysteroscopy for fibroids, endometrial polyps, or uterine septa is associated with a lower mean adhesion score at second-look hysteroscopy at 3 months (mean difference (MD) -1.44, 95 % CI -1.83 to -1.05, < 0.00001, one study, 24 women; this benefit is even larger in women undergoing operative hysteroscopy for intrauterine adhesions(MD -3.30, 95 % CI -3.43 to -3.17, < 0.00001, one study, 19 women). After using any gel following operative hysteroscopy, there are more American Fertility Society 1988 stage I (mild) adhesions (RR 2.81, 95 % CI 1.13 to 7.01, = 0.03, four studies, 79 women). The number needed to treat to benefit is 2 (95 % CI 1 to 4). Similarly there are less' moderate or severe adhesions' at second-look hysteroscopy (RR 0.25, 95 % CI 0.10 to 0.67, = 0.006, four studies, 79 women). The number needed to treat to benefit is 2 (95 % CI 1 to 4) (all very low quality evidence). There are some concerns for the non-methodological quality. Only two trials included infertile women; in the remaining three studies, it is not clear whether and how many participants suffered from infertility. Therefore, the applicability of the findings of the included studies to the target population under study should be questioned. Moreover, only one small trial studied the effects of anti-adhesion barrier gels for the key outcome of pregnancy; the length of follow-up was, however, not specified. More well-designed and adequately powered randomized studies are needed to assess whether the use of any anti-adhesion gel affects the key reproductive outcomes in a target population of infertile women.
本研究旨在评估宫腔镜手术后使用任何抗粘连屏障凝胶治疗与子宫腔异常相关不孕症的效果。妇科医生可能会在宫腔镜手术后对不孕女性使用任何屏障凝胶,以减少新粘连的形成;使用任何屏障凝胶与较轻的新粘连及较低的平均粘连评分相关。然而,应告知不孕女性,目前尚无证据表明使用屏障凝胶能提高活产率或妊娠率。关于流产结局的数据不足。临床前研究表明,使用可生物降解的手术屏障可能会减少术后粘连的形成。人类的观察性研究报告了相互矛盾的结果。我们检索了Cochrane月经紊乱与生育力低下专题注册库(2013年4月10日)、Cochrane对照试验中心注册库(2013年第1期)、MEDLINE(1950年至2013年4月4日)、EMBASE(1974年至2013年4月4日)以及其他试验电子数据库,包括试验注册库、未发表文献来源和参考文献列表。我们手工检索了(1992年1月1日至2013年4月13日);我们还联系了该领域的专家。我们纳入了宫腔镜手术后任何抗粘连屏障凝胶与另一种屏障凝胶、安慰剂或无辅助治疗之间的随机对照比较。主要结局是活产率和二次宫腔镜检查时新粘连的形成。次要结局是妊娠和流产率、平均粘连评分以及二次宫腔镜检查时粘连的严重程度。两位作者独立评估符合纳入标准的研究及其偏倚风险,并提取数据。我们联系了原始研究作者以获取更多信息或其他澄清。五项试验符合纳入标准。对于宫腔镜手术后使用任何屏障凝胶在活产或临床妊娠的关键结局方面是否有益,尚无证据支持(风险比(RR)3.0,95%置信区间(CI)0.35至26,P = 0.32,一项研究,30名女性,证据质量极低);关于流产结局没有数据。宫腔镜手术后使用任何凝胶可降低1至3个月时二次宫腔镜检查时新粘连的发生率(RR 0.65,95% CI 0.45至0.93,P = 0.02,五项研究,372名女性,证据质量极低)。需治疗人数为9(95% CI 5至33)。对于因子宫肌瘤、子宫内膜息肉或子宫纵隔接受宫腔镜手术的女性,使用自交联透明质酸凝胶与3个月时二次宫腔镜检查时较低的平均粘连评分相关(平均差(MD) -1.44,95% CI -1.83至 -1.05,P < 0.00001,一项研究,24名女性;对于因宫腔粘连接受宫腔镜手术的女性,这种益处更大(MD -3.30,95% CI -3.43至 -3.17,P < 0.00001,一项研究,19名女性)。宫腔镜手术后使用任何凝胶后,美国生育协会1988年I期(轻度)粘连更多(RR 2.81,95% CI 1.13至7.01,P = 0.03,四项研究,79名女性)。需治疗人数为2(95% CI 1至4)。同样,二次宫腔镜检查时“中度或重度粘连”较少(RR 0.25,95% CI 0.10至0.67,P = 0.006,四项研究,79名女性)。需治疗人数为2(95% CI 1至4)(所有证据质量极低)。对于非方法学质量存在一些担忧。只有两项试验纳入了不孕女性;在其余三项研究中,不清楚是否以及有多少参与者患有不孕症。因此,纳入研究的结果对所研究的目标人群的适用性应受到质疑。此外,只有一项小型试验研究了抗粘连屏障凝胶对妊娠关键结局的影响;然而,随访时间未明确规定。需要更多设计良好且有足够样本量的随机研究来评估使用任何抗粘连凝胶是否会影响不孕女性目标人群的关键生殖结局。