Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Victoria, BC V8W 1Y2, Canada
Centre for Clinical Epidemiology, Lady Davis Institute, Jewish General Hospital, McGill University, Montreal, Canada.
BMJ. 2014 May 29;348:g3244. doi: 10.1136/bmj.g3244.
To evaluate the incremental increase in new onset diabetes from higher potency statins compared with lower potency statins when used for secondary prevention.
Eight population based cohort studies and a meta-analysis.
Six Canadian provinces and two international databases from the UK and US.
136,966 patients aged ≥ 40 years newly treated with statins between 1 January 1997 and 31 March 2011.
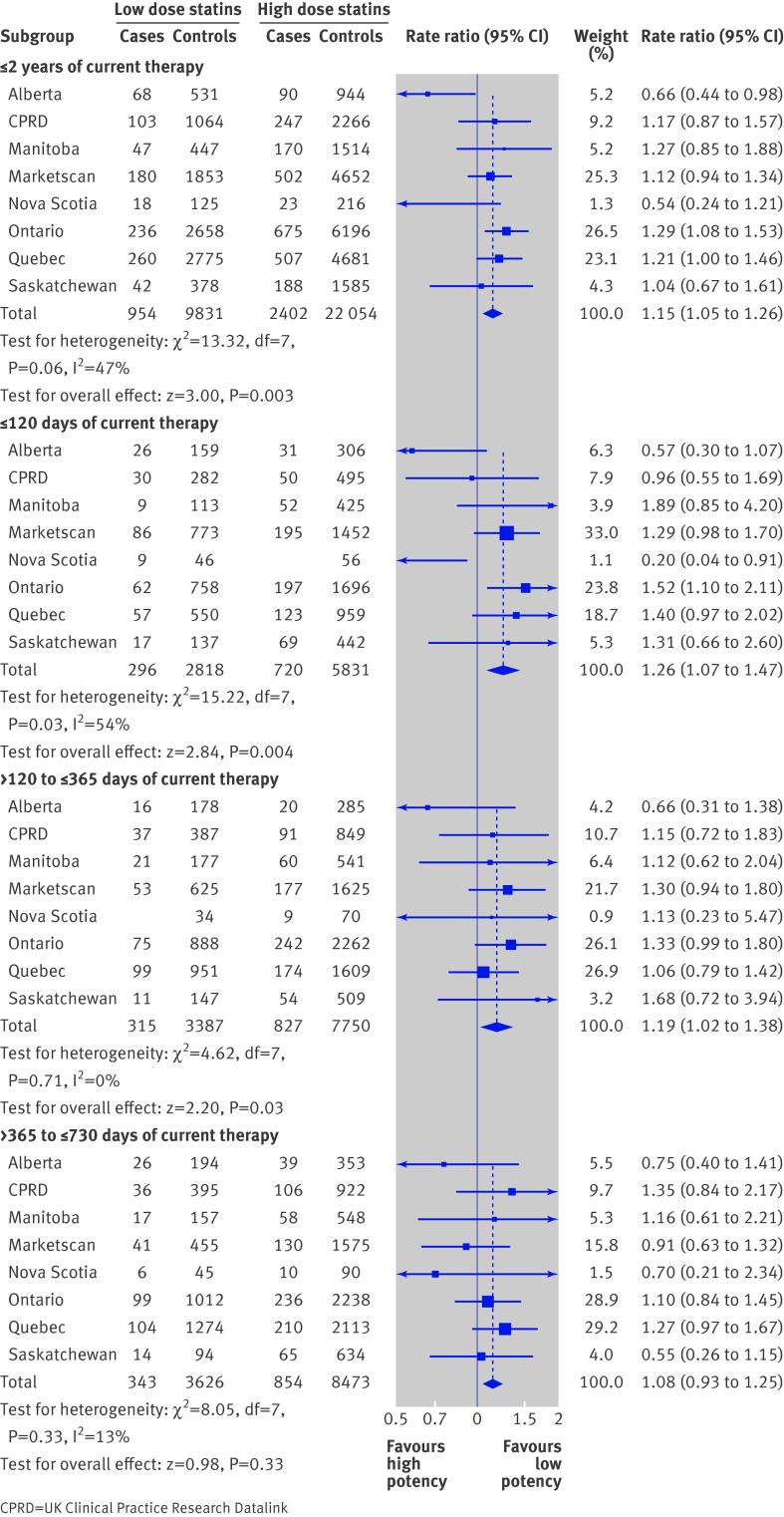
Within each cohort of patients newly prescribed a statin after hospitalisation for a major cardiovascular event or procedure, we performed as-treated, nested case-control analyses to compare diabetes incidence in users of higher potency statins with incidence in users of lower potency statins. Rate ratios of new diabetes events were estimated using conditional logistic regression on different lengths of exposure to higher potency versus lower potency statins; adjustment for confounding was achieved using high dimensional propensity scores. Meta-analytic methods were used to estimate overall effects across sites.
Hospitalisation for new onset diabetes, or a prescription for insulin or an oral antidiabetic drug.
In the first two years of regular statin use, we observed a significant increase in the risk of new onset diabetes with higher potency statins compared with lower potency agents (rate ratio 1.15, 95% confidence interval 1.05 to 1.26). The risk increase seemed to be highest in the first four months of use (rate ratio 1.26, 1.07 to 1.47).
Higher potency statin use is associated with a moderate increase in the risk of new onset diabetes compared with lower potency statins in patients treated for secondary prevention of cardiovascular disease. Clinicians should consider this risk when prescribing higher potency statins in secondary prevention patients.
评估与低效能他汀类药物相比,用于二级预防时,更高效能的他汀类药物会导致新发糖尿病的增量增加。
8 项基于人群的队列研究和一项荟萃分析。
加拿大 6 个省份和来自英国和美国的 2 个国际数据库。
136966 名年龄≥40 岁的患者,在 1997 年 1 月 1 日至 2011 年 3 月 31 日期间因重大心血管事件或操作而住院后首次接受他汀类药物治疗。
在每个新处方他汀类药物治疗的患者队列中,我们对住院后接受更高效能和低效能他汀类药物治疗的患者进行了病例对照嵌套分析,以比较新发生糖尿病的发病率。使用条件逻辑回归比较不同时间暴露于高、低效能他汀类药物的新发糖尿病事件的比率比,通过高维倾向评分进行混杂因素调整。采用荟萃分析方法估计不同地点的总体效果。
新发糖尿病的住院治疗或胰岛素或口服降糖药的处方。
在常规他汀类药物使用的前两年,我们观察到与低效能药物相比,更高效能他汀类药物的新发糖尿病风险显著增加(比值比 1.15,95%置信区间 1.05 至 1.26)。这种风险增加似乎在使用的前四个月最高(比值比 1.26,1.07 至 1.47)。
与低效能他汀类药物相比,在治疗心血管疾病二级预防的患者中,更高效能的他汀类药物的使用与新发糖尿病风险的适度增加相关。临床医生在为二级预防患者开更高效能的他汀类药物时应考虑到这一风险。