Authors' Affiliations: Departments of Molecular Medicine, General Thoracic Surgery, Pulmonary and Critical Care Medicine, Health Sciences Research, and Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota.
Authors' Affiliations: Departments of Molecular Medicine, General Thoracic Surgery, Pulmonary and Critical Care Medicine, Health Sciences Research, and Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MinnesotaAuthors' Affiliations: Departments of Molecular Medicine, General Thoracic Surgery, Pulmonary and Critical Care Medicine, Health Sciences Research, and Laboratory Medicine and Pathology, Mayo Clinic, Rochester, Minnesota.
Cancer Res. 2014 Jun 1;74(11):3157-67. doi: 10.1158/0008-5472.CAN-13-1727.
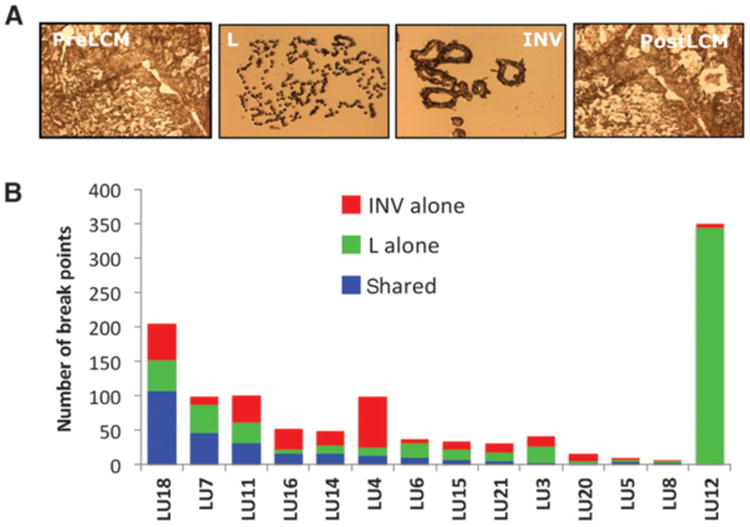
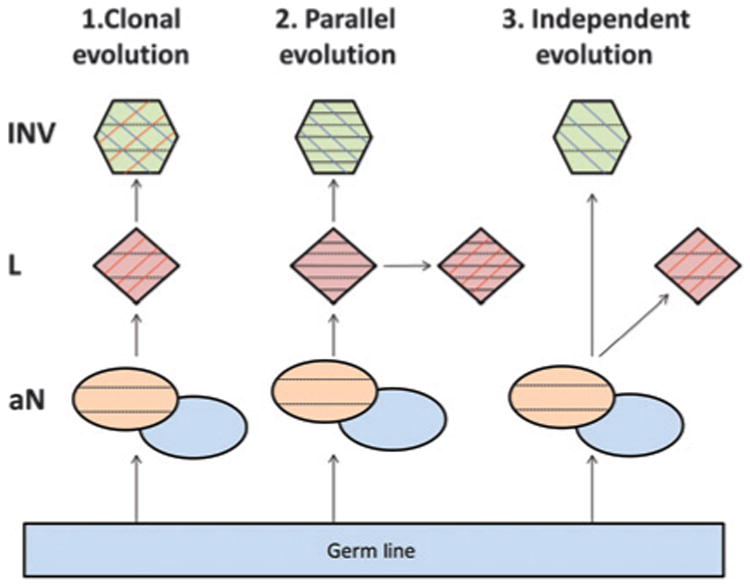
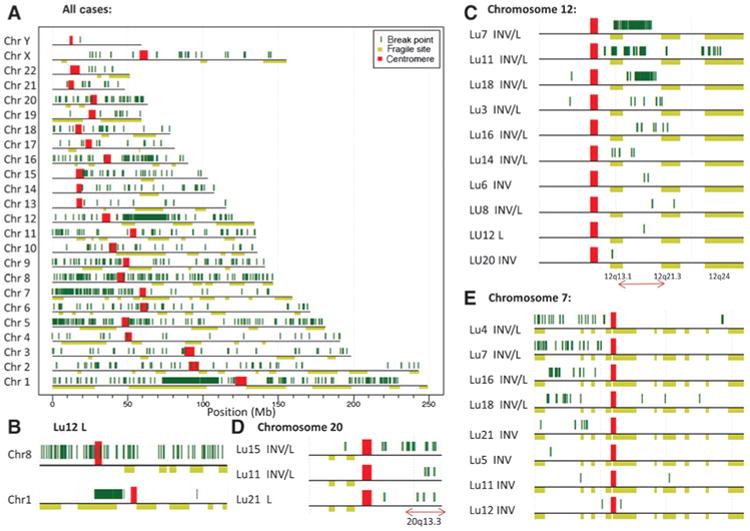
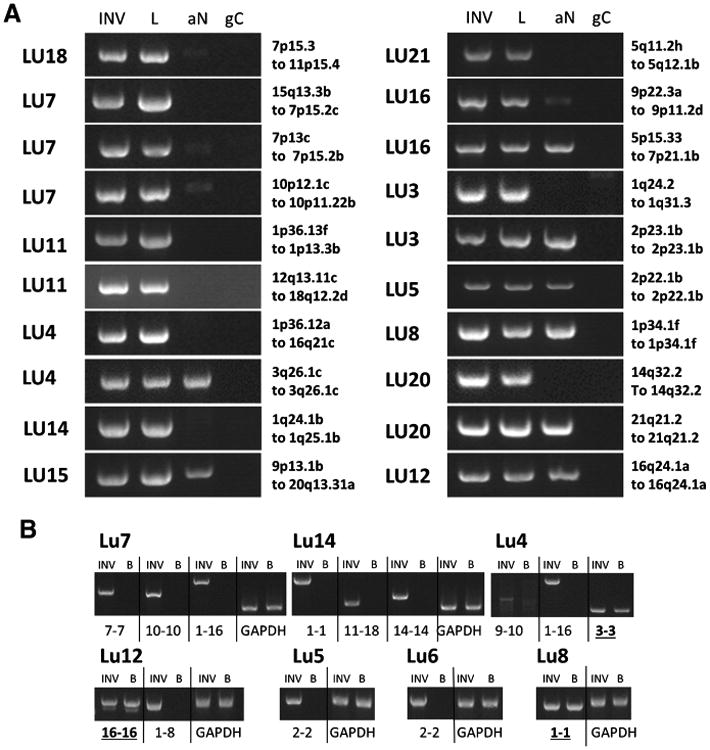
The development of adenocarcinoma of the lung is believed to proceed from in situ disease (adenocarcinoma in situ, AIS) to minimally invasive disease with prominent lepidic growth (minimally invasive adenocarcinoma, MIA), then to fully invasive adenocarcinoma (AD), but direct evidence for this model has been lacking. Because some lung adenocarcinomas show prominent lepidic growth (AD-L), we designed a study to address the lineage relationship between the lepidic (noninvasive) component (L) and the adjacent nonlepidic growth component representing invasive disease within individual tumors. Lineage relationships were evaluated by next-generation DNA sequencing to define large genomic rearrangements in microdissected tissue specimens collected by laser capture. We found a strong lineage relationship between the majority of adjacent lepidic and invasive components, supporting a putative AIS-AD transition. Notably, many rearrangements were detected in the less aggressive lepidic component, although the invasive component exhibited an overall higher rate of genomic rearrangement. Furthermore, a significant number of genomic rearrangements were present in histologically normal lung adjacent to tumor, but not in host germline DNA, suggesting field defects restricted to zonal regions near a tumor. Our results offer a perspective on the genetic pathogenesis underlying adenocarcinoma development and its clinical management.
肺腺癌的发展被认为是从原位疾病(原位腺癌,AIS)进展为具有明显贴壁生长的微创疾病(微创腺癌,MIA),然后进展为完全浸润性腺癌(AD),但该模型的直接证据一直缺乏。因为一些肺腺癌表现出明显的贴壁生长(AD-L),所以我们设计了一项研究来解决单个肿瘤中相邻的贴壁(非侵袭性)成分(L)与代表侵袭性疾病的相邻非贴壁生长成分之间的谱系关系。通过下一代 DNA 测序来评估谱系关系,以定义通过激光捕获收集的显微解剖组织标本中的大基因组重排。我们发现大多数相邻的贴壁和侵袭性成分之间存在很强的谱系关系,支持 AIS-AD 转化的假设。值得注意的是,许多重排在侵袭性成分中检测到,尽管侵袭性成分总体上具有更高的基因组重排率。此外,在肿瘤旁的组织学正常肺中存在大量的基因组重排,但在宿主种系 DNA 中不存在,这表明肿瘤附近区域的局部缺陷。我们的结果提供了一个关于腺癌发展及其临床管理的遗传发病机制的视角。