Molecular Medicine and Biomarker Discovery Program, Center for Individualized Medicine, Mayo Clinic, Rochester, MN.
Oncology, Mayo Clinic, Rochester, MN; Laboratory Medicine and Pathology, Rochester, MN.
Mayo Clin Proc. 2020 Feb;95(2):306-318. doi: 10.1016/j.mayocp.2019.07.019. Epub 2019 Nov 2.
To select optimal therapies based on the detection of actionable genomic alterations in tumor samples is a major challenge in precision medicine.
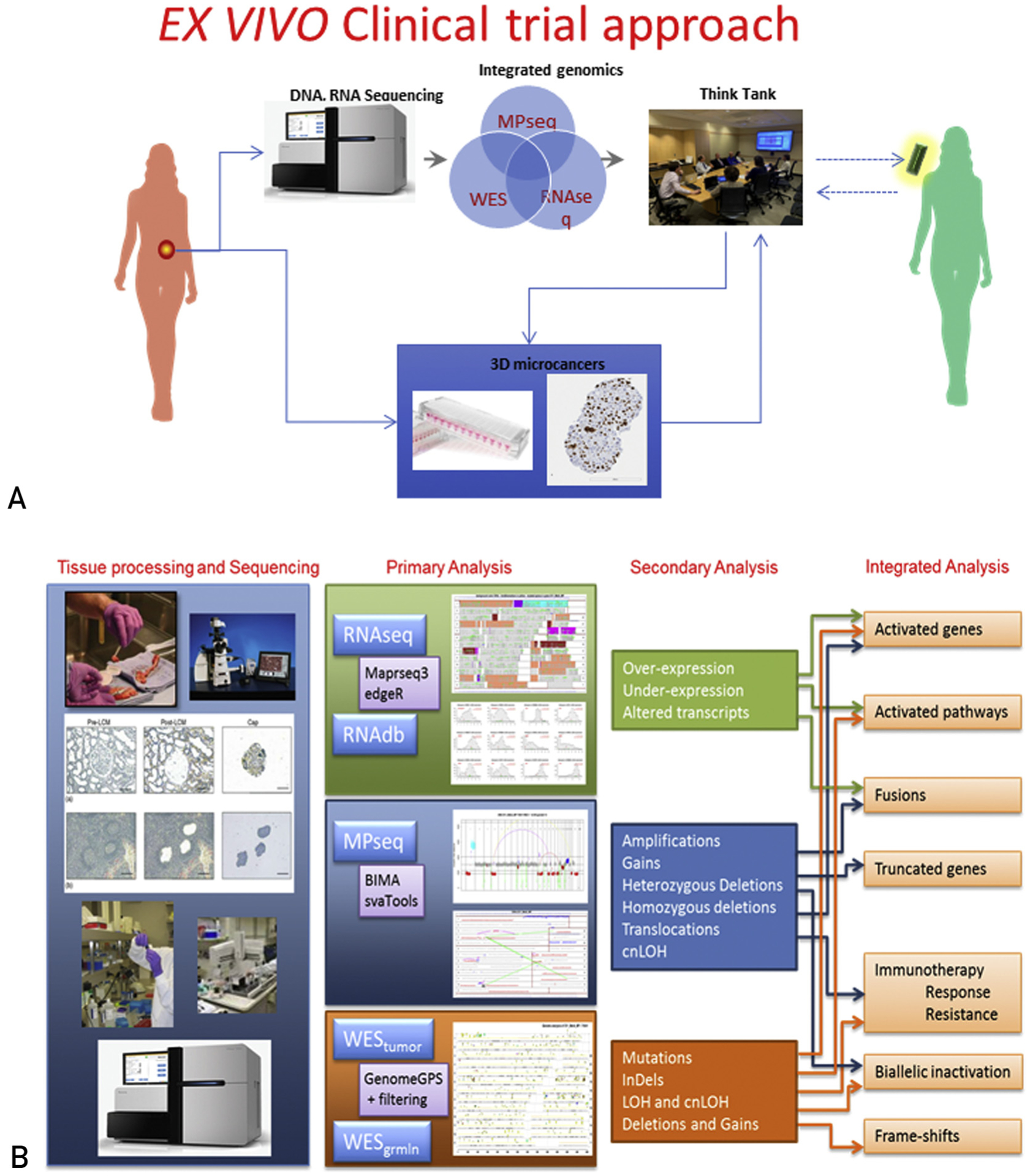
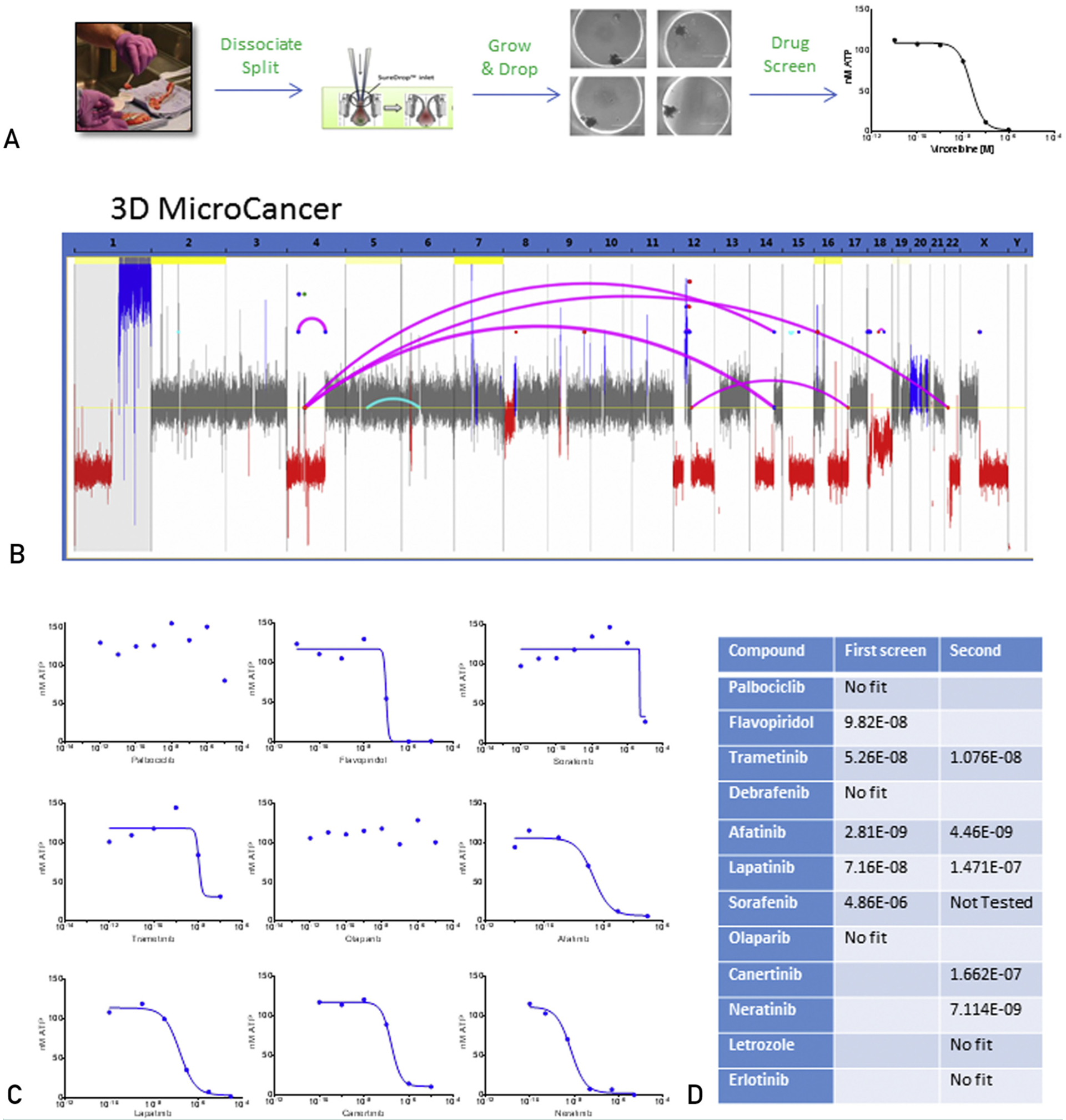
We describe an effective process (opened December 1, 2017) that combines comprehensive genomic and transcriptomic tumor profiling, custom algorithms and visualization software for data integration, and preclinical 3-dimensiona ex vivo models for drug screening to assess response to therapeutic agents targeting specific genomic alterations. The process was applied to a patient with widely metastatic, weakly hormone receptor positive, HER2 nonamplified, infiltrating lobular breast cancer refractory to standard therapy.
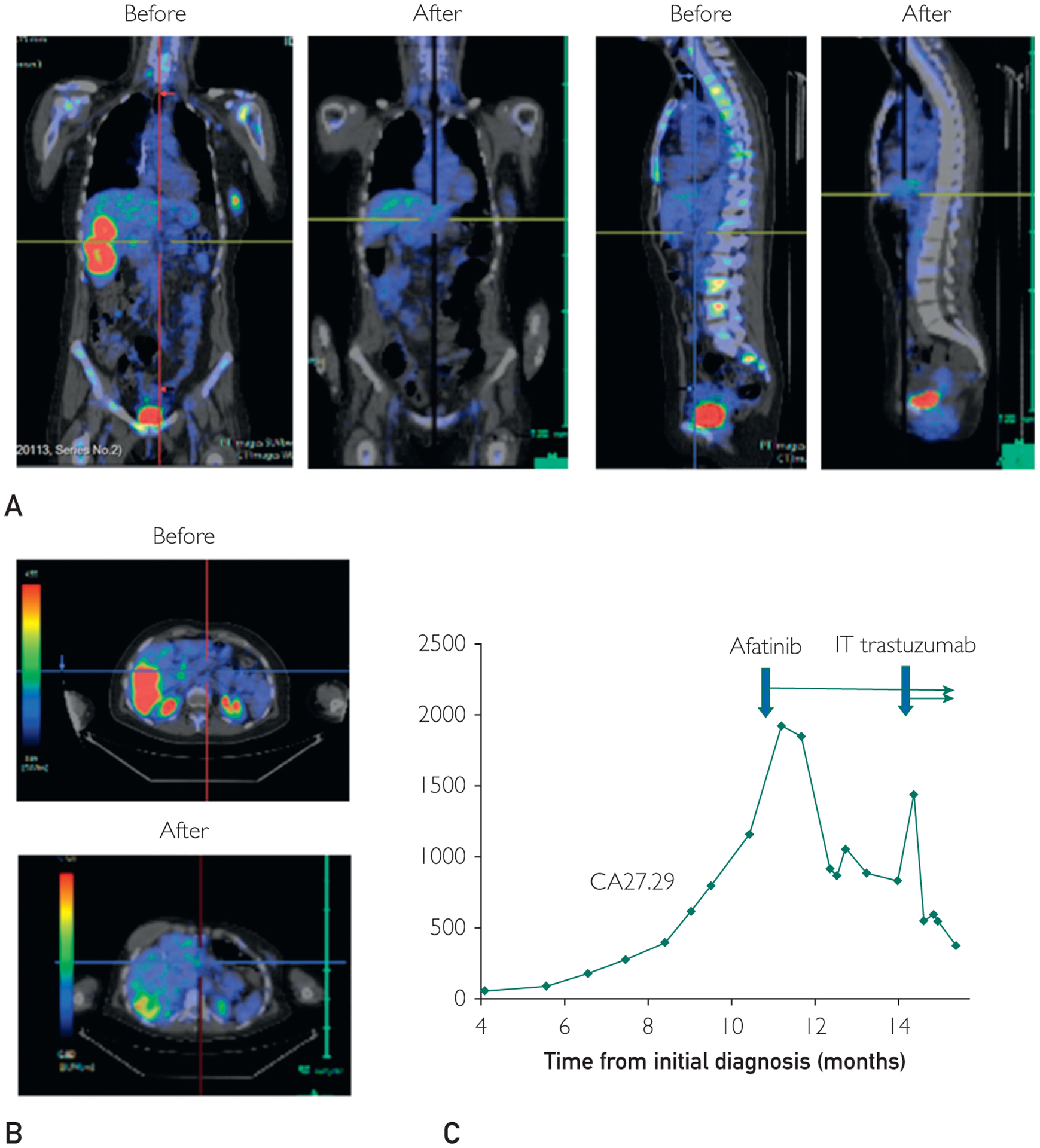
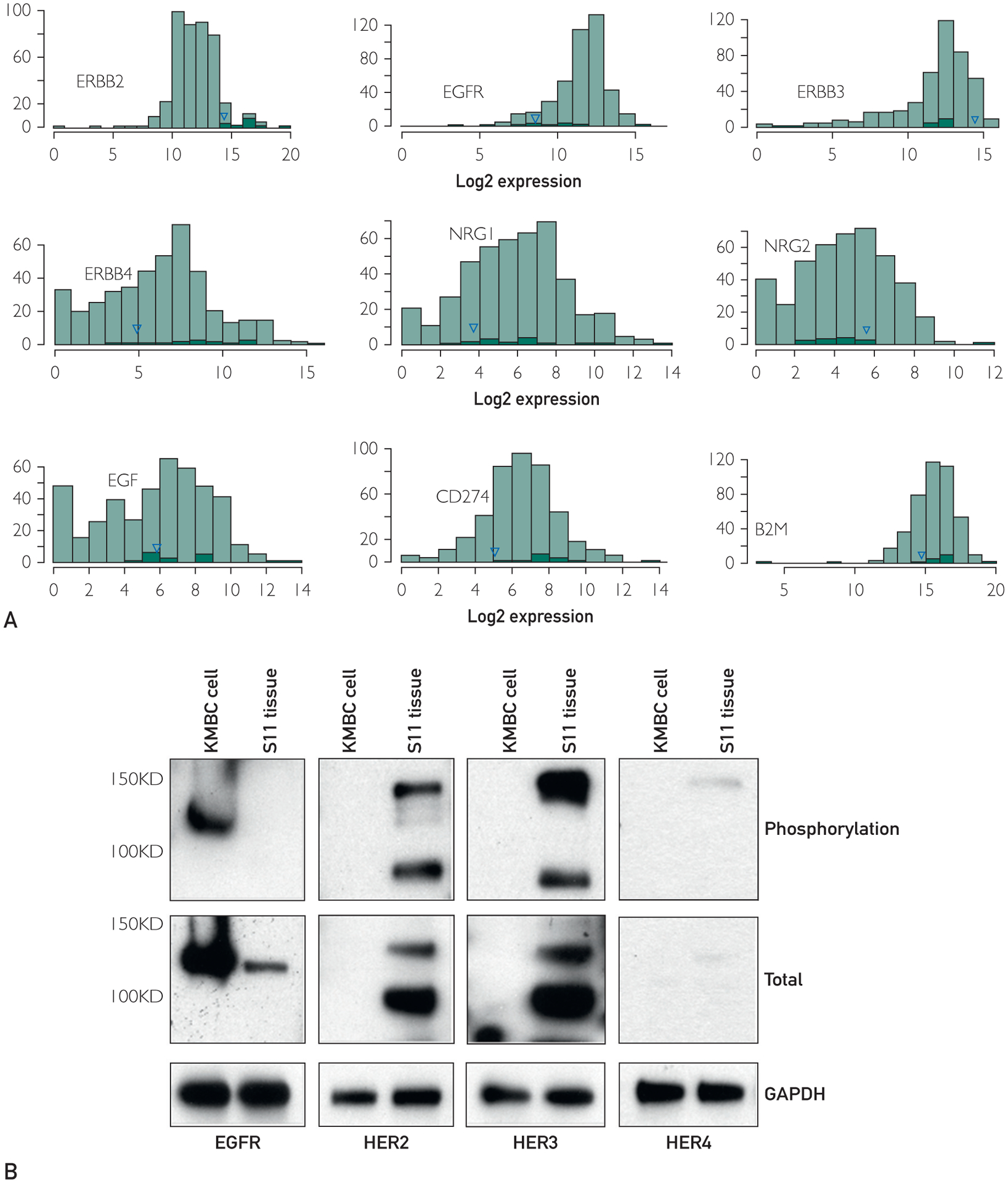
Clinical testing of liver metastasis identified BRIP1, NF1, CDH1, RB1, and TP53 mutations pointing to potential therapies including PARP, MEK/RAF, and CDK inhibitors. The comprehensive genomic analysis identified 395 mutations and several structural rearrangements that resulted in loss of function of 36 genes. Meta-analysis revealed biallelic inactivation of TP53, CDH1, FOXA1, and NIN, whereas only one allele of NF1 and BRIP1 was mutated. A novel ERBB2 somatic mutation of undetermined significance (P702L), high expression of both mutated and wild-type ERBB2 transcripts, high expression of ERBB3, and a LITAF-BCAR4 fusion resulting in BCAR4 overexpression pointed toward ERBB-related therapies. Ex vivo analysis validated the ERBB-related therapies and invalidated therapies targeting mutations in BRIP1 and NF1. Systemic patient therapy with afatinib, a HER1/HER2/HER4 small molecule inhibitor, resulted in a near complete radiographic response by 3 months.
Unlike clinical testing, the combination of tumor profiling, data integration, and functional validation accurately assessed driver alterations and predicted effective treatment.
根据肿瘤样本中可操作的基因组改变来选择最佳治疗方法是精准医学的主要挑战。
我们描述了一种有效的流程(于 2017 年 12 月 1 日开放),该流程结合了全面的基因组和转录组肿瘤分析、用于数据整合的定制算法和可视化软件,以及用于药物筛选的三维离体模型,以评估针对特定基因组改变的治疗药物的反应。该流程应用于一位广泛转移、弱激素受体阳性、HER2 非扩增、浸润性小叶乳腺癌的患者,该患者对标准治疗有抗药性。
对肝转移的临床检测鉴定出 BRIP1、NF1、CDH1、RB1 和 TP53 突变,提示可能的治疗方法包括 PARP、MEK/RAF 和 CDK 抑制剂。全面的基因组分析鉴定出 395 个突变和几个结构重排,导致 36 个基因的功能丧失。荟萃分析显示 TP53、CDH1、FOXA1 和 NIN 的双等位基因失活,而 NF1 和 BRIP1 只有一个等位基因突变。一个新的 ERBB2 体细胞突变意义不明(P702L),突变和野生型 ERBB2 转录本的高表达,ERBB3 的高表达,以及导致 BCAR4 过表达的 LITAF-BCAR4 融合,提示与 ERBB 相关的治疗。离体分析验证了与 ERBB 相关的治疗方法,并否定了针对 BRIP1 和 NF1 突变的治疗方法。系统的患者用 afatinib(一种 HER1/HER2/HER4 小分子抑制剂)治疗,3 个月后接近完全的影像学反应。
与临床检测不同,肿瘤分析、数据整合和功能验证的结合准确地评估了驱动改变,并预测了有效的治疗方法。