Cavalera Michele, Wang Junhong, Frangogiannis Nikolaos G
Division of Cardiology, Department of Medicine, The Wilf Cardiovascular Research Institute, Albert Einstein College of Medicine, Bronx, New York.
Division of Cardiology, Department of Medicine, The Wilf Cardiovascular Research Institute, Albert Einstein College of Medicine, Bronx, New York.
Transl Res. 2014 Oct;164(4):323-35. doi: 10.1016/j.trsl.2014.05.001. Epub 2014 May 10.
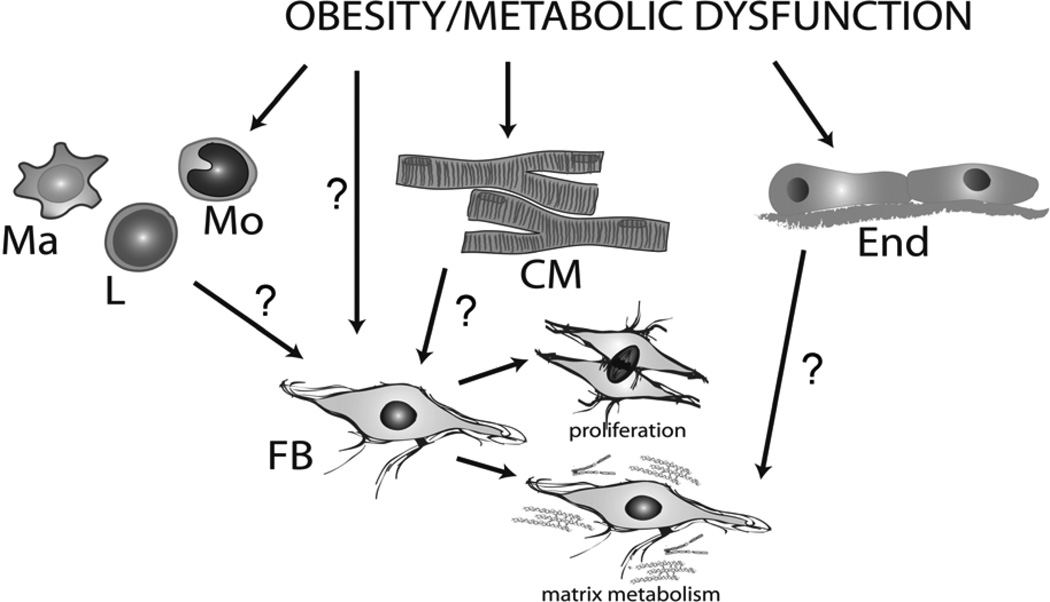
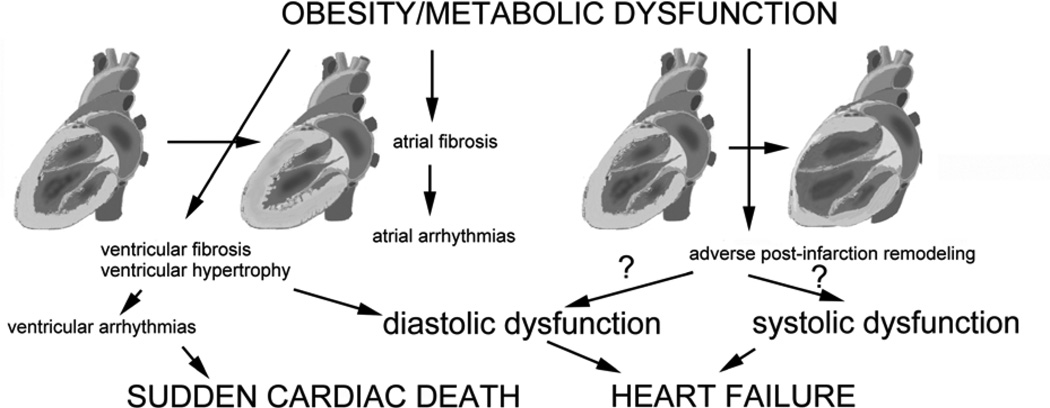
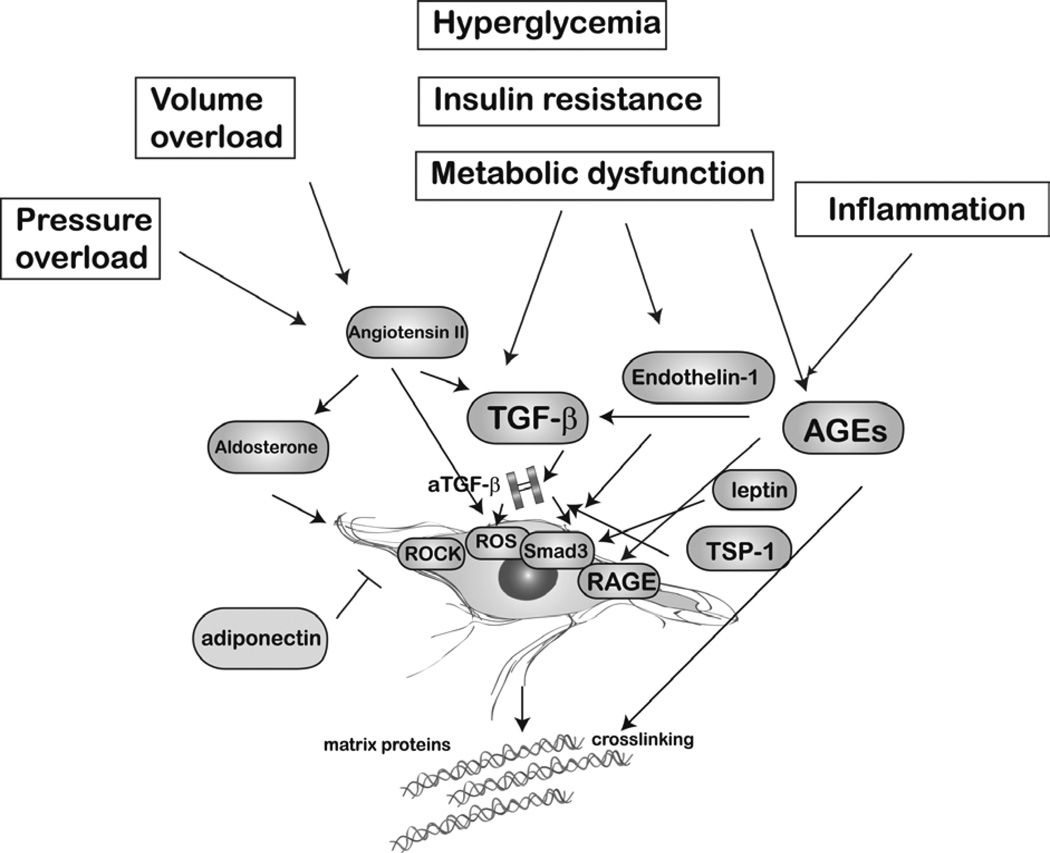
Cardiac fibrosis is strongly associated with obesity and metabolic dysfunction and may contribute to the increased incidence of heart failure, atrial arrhythmias, and sudden cardiac death in obese subjects. This review discusses the evidence linking obesity and myocardial fibrosis in animal models and human patients, focusing on the fundamental pathophysiological alterations that may trigger fibrogenic signaling, the cellular effectors of fibrosis, and the molecular signals that may regulate the fibrotic response. Obesity is associated with a wide range of pathophysiological alterations (such as pressure and volume overload, metabolic dysregulation, neurohumoral activation, and systemic inflammation); their relative role in mediating cardiac fibrosis is poorly defined. Activation of fibroblasts likely plays a major role in obesity-associated fibrosis; however, inflammatory cells, cardiomyocytes, and vascular cells may also contribute to fibrogenic signaling. Several molecular processes have been implicated in regulation of the fibrotic response in obesity. Activation of the renin-angiotensin-aldosterone system, induction of transforming growth factor β, oxidative stress, advanced glycation end-products, endothelin 1, Rho-kinase signaling, leptin-mediated actions, and upregulation of matricellular proteins (such as thrombospondin 1) may play a role in the development of fibrosis in models of obesity and metabolic dysfunction. Moreover, experimental evidence suggests that obesity and insulin resistance profoundly affect the fibrotic and remodeling response after cardiac injury. Understanding the pathways implicated in obesity-associated fibrosis may lead to the development of novel therapies to prevent heart failure and attenuate postinfarction cardiac remodeling in patients with obesity.
心脏纤维化与肥胖和代谢功能障碍密切相关,可能导致肥胖个体心力衰竭、房性心律失常和心源性猝死的发病率增加。本综述讨论了动物模型和人类患者中肥胖与心肌纤维化之间联系的证据,重点关注可能触发纤维化信号传导的基本病理生理改变、纤维化的细胞效应器以及可能调节纤维化反应的分子信号。肥胖与多种病理生理改变有关(如压力和容量超负荷、代谢失调、神经体液激活和全身炎症);它们在介导心脏纤维化中的相对作用尚不清楚。成纤维细胞的激活可能在肥胖相关纤维化中起主要作用;然而,炎症细胞、心肌细胞和血管细胞也可能促成纤维化信号传导。肥胖中纤维化反应的调节涉及几个分子过程。肾素-血管紧张素-醛固酮系统的激活、转化生长因子β的诱导、氧化应激、晚期糖基化终产物、内皮素1、Rho激酶信号传导、瘦素介导的作用以及基质细胞蛋白(如血小板反应蛋白1)的上调可能在肥胖和代谢功能障碍模型的纤维化发展中起作用。此外,实验证据表明,肥胖和胰岛素抵抗深刻影响心脏损伤后的纤维化和重塑反应。了解肥胖相关纤维化所涉及的途径可能会导致开发新的疗法,以预防肥胖患者的心力衰竭并减轻心肌梗死后的心脏重塑。