Laroni Alice, Gandoglia Ilaria, Solaro Claudio, Ribizzi Giuseppe, Tassinari Tiziana, Pizzorno Matteo, Parodi Sergio, Baldassarre Giovanna, Rilla Maria Teresa, Venturi Simonetta, Capello Elisabetta, Sormani Maria Pia, Uccelli Antonio, Mancardi Giovanni Luigi
Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Largo Daneo 3, 16132 Genova, Italy.
BMC Neurol. 2014 May 12;14:103. doi: 10.1186/1471-2377-14-103.
Optimal patient selection would improve the risk-benefit ratio of natalizumab treatment for relapsing-remitting multiple sclerosis (RR MS). Clinical features of subjects responding to natalizumab have not been univocally recognized.
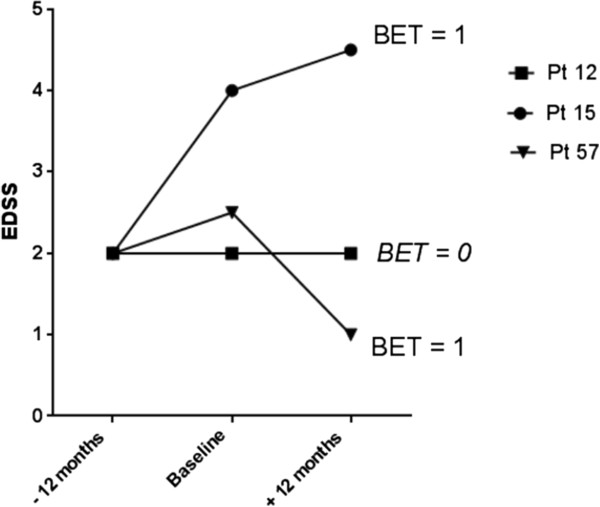
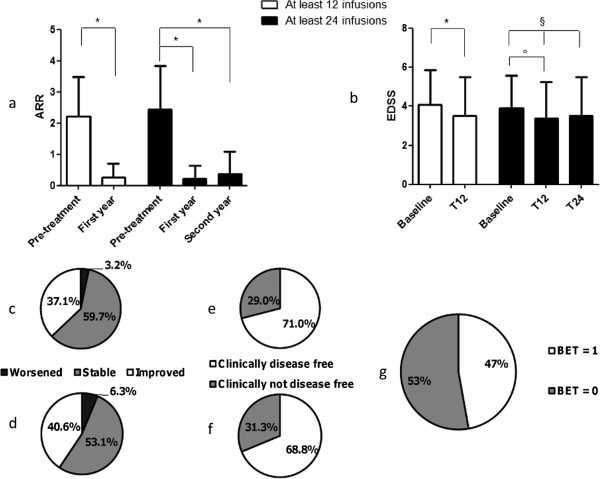
Longitudinal data on RR MS patients treated with natalizumab in Liguria, Italy are reported. Predictors of relapse occurrence and disability improvement were analyzed with a logistic regression method in subjects treated for one year (N = 62). A new score, called "Better EDSS Trend (BET)", was devised to describe the impact of the treatment on disability. Changes in annualized relapse rate (ARR) and Expanded Disability Status Scale (EDSS) after one and two years and proportion of disease-free patients were evaluated.
Previous EDSS worsening plus ARR ≥ 2 increased the risk of relapse during the treatment [Odds Ratio (OR) 4.12, P = 0.04], but this was not associated with an increase in disability at one year. EDSS 3.0-3.5 or high disease activity were associated with neurological improvement in the first year of treatment (respectively OR 5.78, P = 0.05 and OR 4.80, P = 0.05). Positive BET score, i.e. improvement in the disability trend, was observed in 40.3% of patients, and correlated with high ARR in the year before treatment (OR 1.69, P = 0.03).
Subjects with EDSS 3.0-3.5 and those with very active disease in the year before treatment are most likely to improve in neurological function under natalizumab. A relapse in the first year of treatment is associated to high pre-treatment disease activity; however, since the occurrence of a relapse did not have a negative impact on clinical improvement at one year, we suggest that it should not lead to treatment discontinuation. We propose BET as an additional endpoint of treatment response in MS.
最佳的患者选择将改善那他珠单抗治疗复发缓解型多发性硬化症(RR MS)的风险效益比。对那他珠单抗有反应的受试者的临床特征尚未得到明确认识。
报告了意大利利古里亚接受那他珠单抗治疗的RR MS患者的纵向数据。采用逻辑回归方法分析了治疗一年的受试者(N = 62)复发发生和残疾改善的预测因素。设计了一个名为“更好的EDSS趋势(BET)”的新评分来描述治疗对残疾的影响。评估了一年和两年后的年化复发率(ARR)和扩展残疾状态量表(EDSS)的变化以及无病患者的比例。
既往EDSS恶化加上ARR≥2会增加治疗期间复发的风险[比值比(OR)4.12,P = 0.04],但这与一年时残疾增加无关。EDSS 3.0 - 3.5或高疾病活动度与治疗第一年的神经功能改善相关(分别为OR 5.78,P = 0.05和OR 4.80,P = 0.05)。40.3%的患者观察到BET评分呈阳性,即残疾趋势改善,且与治疗前一年的高ARR相关(OR 1.69,P = 0.03)。
EDSS为3.0 - 3.5的受试者以及治疗前一年疾病非常活跃的受试者在接受那他珠单抗治疗时最有可能改善神经功能。治疗第一年的复发与治疗前的高疾病活动度相关;然而,由于复发的发生对一年时的临床改善没有负面影响,我们建议不应导致治疗中断。我们建议将BET作为MS治疗反应的一个额外终点。