the 1st Affiliated Hospital of Wenzhou Medical College.
J Appl Clin Med Phys. 2014 May 8;15(3):93–101. doi: 10.1120/jacmp.v15i3.4641.
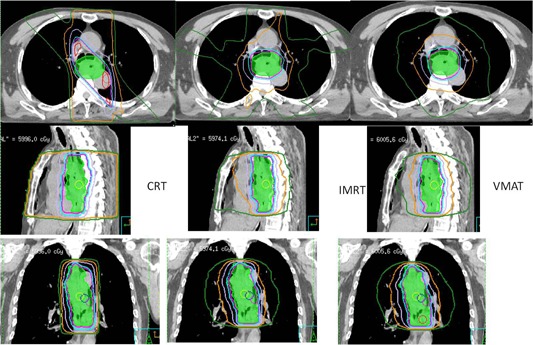
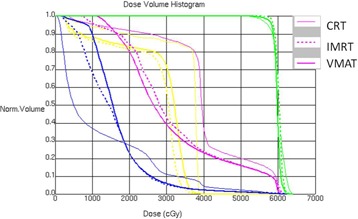
The purpose of this study is to investigate the dosimetric differences among conformal radiotherapy (CRT), intensity-modulated radiotherapy (IMRT), and volumetric-modulated radiotherapy (VMAT) in the treatment of middle thoracic esophageal cancer, and determine the most appropriate treatment modality. IMRT and one-arc VMAT plans were generated for eight middle thoracic esophageal cancer patients treated previous with CRT. The planning target volume (PTV) coverage and protections on organs at risk of three planning schemes were compared. All plans have sufficient PTV coverage and no significant differences were observed, except for the conformity and homogeneity. The lung V5, V10, and V13 in CRT were 47.9% ± 6.1%, 36.5% ± 4.6%, and 33.2% ± 4.2%, respectively, which were greatly increased to 78.2% ± 13.7% (p < 0.01), 80.8% ± 14.9% (p < 0.01), 48.4% ± 8.2% (p = 0.05) in IMRT and 58.6% ± 10.5% (p = 0.03), 67.7% ± 14.0% (p < 0.01), and 53.0% ± 10.1% (p < 0.01) in VMAT, respectively. The lung V20 (p = 0.03) in VMAT and the V30 (p = 0.04) in IMRT were lower than those in CRT. Both IMRT and VMAT achieved a better protection on heart. However, the volumes of the healthy tissue outside of PTV irradiated by a low dose were higher for IMRT and VMAT. IMRT and VMAT also had a higher MU, optimization time, and delivery time compared to CRT. In conclusion, all CRT, IMRT, and VMAT plans are able to meet the prescription and there is no clear distinction on PTV coverage. IMRT and VMAT can only decrease the volume of lung and heart receiving a high dose, but at a cost of delivering low dose to more volume of lung and normal tissues. CRT is still a feasible option for middle thoracic esophageal cancer radiotherapy, especially for the cost-effective consideration.
本研究旨在探讨适形放疗(CRT)、调强放疗(IMRT)和容积调强放疗(VMAT)在治疗中胸段食管癌中的剂量学差异,并确定最合适的治疗方式。对 8 例接受 CRT 治疗的中胸段食管癌患者生成了 IMRT 和单弧 VMAT 计划。比较了三种计划方案的靶区(PTV)覆盖和危及器官的保护。所有计划方案均有足够的 PTV 覆盖,除了适形性和均匀性外,没有观察到明显差异。CRT 中肺 V5、V10 和 V13 分别为 47.9%±6.1%、36.5%±4.6%和 33.2%±4.2%,在 IMRT 中分别增加到 78.2%±13.7%(p<0.01)、80.8%±14.9%(p<0.01)和 48.4%±8.2%(p=0.05),在 VMAT 中分别增加到 58.6%±10.5%(p=0.03)、67.7%±14.0%(p<0.01)和 53.0%±10.1%(p<0.01)。VMAT 中的肺 V20(p=0.03)和 IMRT 中的 V30(p=0.04)均低于 CRT。IMRT 和 VMAT 均能更好地保护心脏。然而,低剂量照射的 PTV 外健康组织的体积对于 IMRT 和 VMAT 来说更高。与 CRT 相比,IMRT 和 VMAT 的 MU、优化时间和输送时间也更高。综上所述,所有 CRT、IMRT 和 VMAT 计划均能满足处方要求,在 PTV 覆盖方面没有明显差异。IMRT 和 VMAT 虽然可以降低肺和心脏接受高剂量的体积,但代价是将低剂量传递到更多的肺和正常组织。CRT 仍然是中胸段食管癌放疗的可行选择,特别是在考虑成本效益的情况下。