Nelson Kyle A, Garbutt Jane M, Wallendorf Michael J, Trinkaus Kathryn M, Strunk Robert C
Department of Emergency Medicine, Boston Children's Hospital , Boston , USA .
J Asthma. 2014 Nov;51(9):907-12. doi: 10.3109/02770903.2014.927483. Epub 2014 Jun 9.
To examine the association between numbers of primary care provider (PCP) visits for asthma monitoring (AM) over time and acute asthma visits in the emergency department (ED) and at the PCP for Medicaid-insured children.
We prospectively enrolled 2-10 years old children during ED asthma visits. We audited hospital and PCP records for each subject for three consecutive years. We excluded subjects also receiving care from asthma subspecialists. PCP AM visits were those with documentation that suggested discussion of asthma management but no acute asthma symptoms or findings. PCP "Acute Asthma" visits were those with documentation of acute asthma symptoms or findings, regardless of treatment. ED asthma visits were those with documented asthma treatment. Generalized liner models were used to analyze the association between numbers of AM visits and acute asthma visits to the ED and PCP.
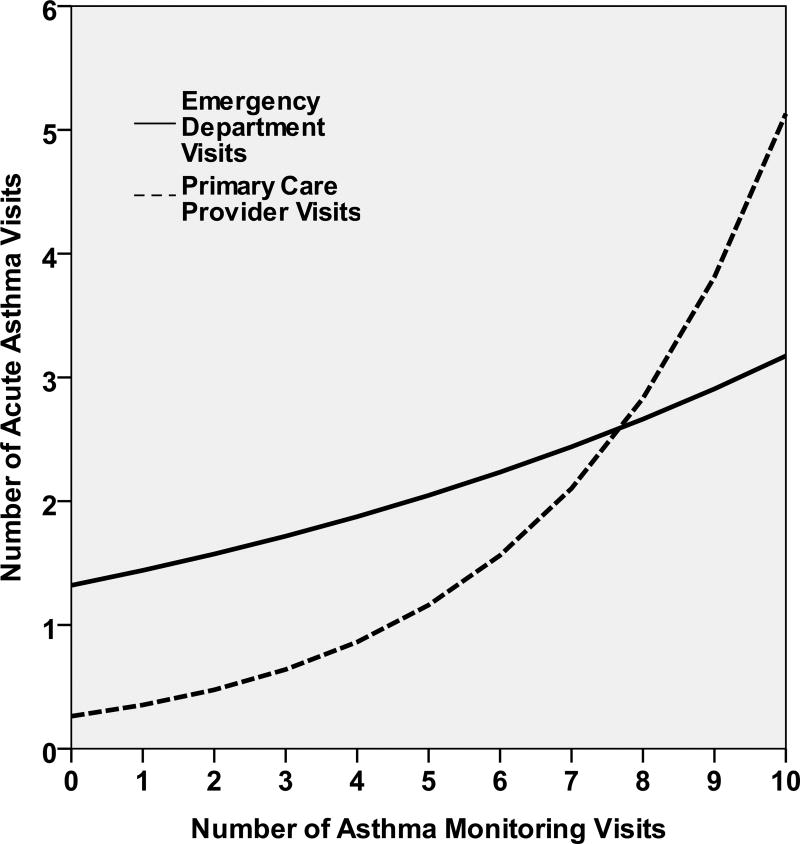
One hundred three subjects were analyzed. Over the 3 years, the mean number of AM visits/child was 2.5 ± 2.3 (standard deviation), range 0-10. Only 50% of subjects had at least 1 PCP visit with an asthma controller medication documented. The mean number of ED asthma visits/child was 3.2 ± 2.8; range 1-18. The mean number of PCP Acute Asthma visits/child was 0.7 ± 1.6; range 0-11. Increasing AM visits was associated with more ED visits (estimate 0.088; 95% CI 0.001, 0.174), and more PCP Acute Asthma visits (estimate 0.297; 95% CI 0.166, 0.429). Increasing PCP visits for any diagnosis was not associated with ED visits (estimate 0.021; 95% CI -0.018, 0.06).
Asthma monitoring visits and documented controller medication for these urban Medicaid-insured children occurred infrequently over 3 years, and having more asthma monitoring visits was not associated with fewer ED or PCP acute asthma visits.
研究医疗补助保险儿童随时间推移因哮喘监测(AM)而进行的初级保健提供者(PCP)就诊次数与急诊科(ED)及PCP处急性哮喘就诊次数之间的关联。
我们在ED哮喘就诊期间前瞻性纳入了2至10岁的儿童。我们连续三年审核了每个受试者的医院和PCP记录。我们排除了同时还接受哮喘专科医生治疗的受试者。PCP的AM就诊是指那些有文件记录表明讨论了哮喘管理但无急性哮喘症状或体征的就诊。PCP的“急性哮喘”就诊是指那些有急性哮喘症状或体征记录的就诊,无论是否接受治疗。ED哮喘就诊是指那些有哮喘治疗记录的就诊。使用广义线性模型分析AM就诊次数与ED及PCP处急性哮喘就诊次数之间的关联。
对103名受试者进行了分析。在这3年中,每个儿童的AM就诊平均次数为2.5±2.3(标准差),范围为0至10次。只有50%的受试者至少有1次有哮喘控制药物记录的PCP就诊。每个儿童的ED哮喘就诊平均次数为3.2±2.8次;范围为1至18次。每个儿童的PCP急性哮喘就诊平均次数为0.7±1.6次;范围为0至11次。AM就诊次数增加与更多的ED就诊相关(估计值0.088;95%置信区间0.001,0.174),以及更多的PCP急性哮喘就诊相关(估计值0.297;95%置信区间0.166,0.429)。因任何诊断而增加的PCP就诊次数与ED就诊无关(估计值0.021;95%置信区间-0.018,0.06)。
在这3年中,这些城市医疗补助保险儿童的哮喘监测就诊和有记录的控制药物使用情况并不常见,且更多的哮喘监测就诊次数与较少的ED或PCP急性哮喘就诊次数无关。