Silva Soraia Aparecida da, Valácio Reginaldo Aparecido, Botelho Flávia Carvalho, Amaral Carlos Faria Santos
Hospital Odilon Behrens, Belo Horizonte, MG, Brasil.
Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brasil.
Rev Saude Publica. 2014 Apr;48(2):314-21. doi: 10.1590/s0034-8910.2014048004971.
To analyze the causes of delay in hospital discharge of patients admitted to internal medicine wards.
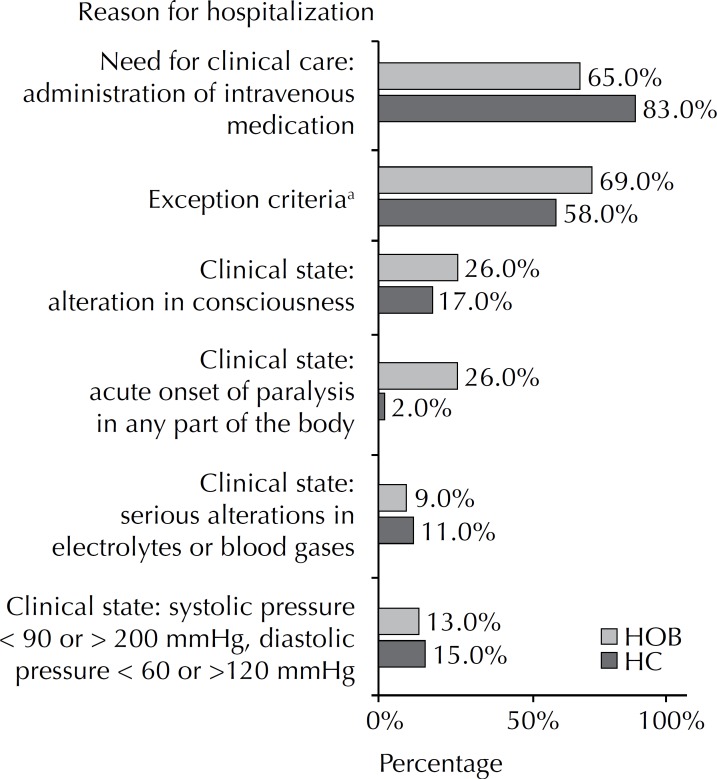
We reviewed 395 medical records of consecutive patients admitted to internal medicine wards of two public teaching hospitals: Hospital das Clínicas of the Universidade Federal de Minas Gerais and Hospital Odilon Behrens. The Appropriateness Evaluation Protocol was used to define the moment at which notes in the medical records indicated hospital stay was no longer appropriate and patients could be discharged. The interval between this estimated time and actual discharge was defined as the total number of days of delay in hospital discharge. An instrument was used to systematically categorize reasons for delay in hospital discharge and frequencies were analyzed.
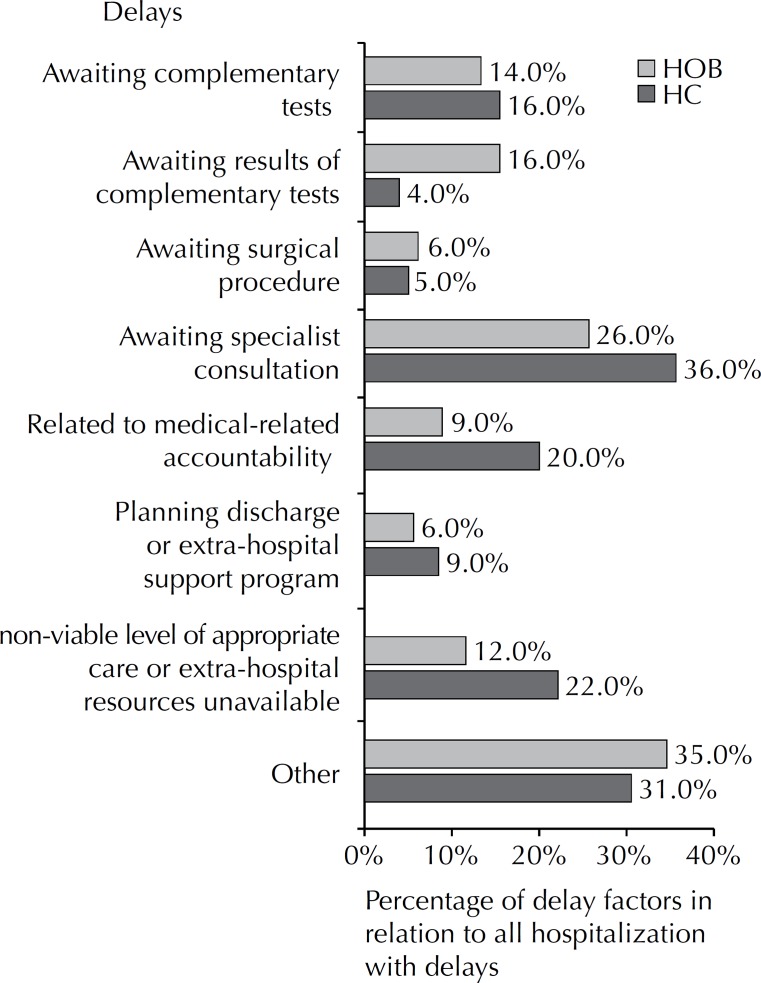
Delays in discharge occurred in 60.0% of 207 hospital admissions in the Hospital das Clínicas and in 58.0% of 188 hospital admissions in the Hospital Odilon Behrens. Mean delay per patient was 4.5 days in the former and 4.1 days in the latter, corresponding to 23.0% and 28.0% of occupancy rates in each hospital, respectively. The main reasons for delay in the two hospitals were, respectively, waiting for complementary tests (30.6% versus 34.7%) or for results of performed tests to be released (22.4% versus 11.9%) and medical-related accountability (36.2% versus 26.1%) which comprised delays in discussing the clinical case and in clinical decision making and difficulties in providing specialized consultation (20.4% versus 9.1%).
Both hospitals showed a high percentage of delay in hospital discharge. The delays were mainly related to processes that could be improved by interventions by care teams and managers. The impact on mean length of stay and hospital occupancy rates was significant and troubling in a scenario of relative shortage of beds and long waiting lists for hospital admission.
分析内科病房患者延迟出院的原因。
我们回顾了两家公立教学医院内科病房连续收治患者的395份病历:米纳斯吉拉斯联邦大学临床医院和奥迪隆·贝伦医院。采用适当性评估方案来确定病历记录显示住院不再合适且患者可以出院的时刻。该估计时间与实际出院之间的间隔被定义为延迟出院的总天数。使用一种工具对延迟出院的原因进行系统分类,并分析其频率。
临床医院207例住院患者中有60.0%出现延迟出院,奥迪隆·贝伦医院188例住院患者中有58.0%出现延迟出院。前者每位患者的平均延迟天数为4.5天,后者为4.1天,分别占各医院床位占用率的23.0%和28.0%。两家医院延迟出院的主要原因分别是等待补充检查(30.6%对34.7%)或等待已进行检查的结果发布(22.4%对11.9%)以及医疗相关责任(36.2%对26.1%),其中包括临床病例讨论和临床决策的延迟以及提供专科会诊的困难(20.4%对9.1%)。
两家医院延迟出院的比例都很高。延迟主要与护理团队和管理人员的干预可改善的流程有关。在床位相对短缺和住院等待名单较长的情况下,对平均住院时间和医院床位占用率的影响是显著且令人担忧的。