Ta Casey N, Eghtedari Mohammad, Mattrey Robert F, Kono Yuko, Kummel Andrew C
From the *Department of Electrical and Computer Engineering, University of California, San Diego, La Jolla; †University of Texas MD Anderson Cancer Center, Houston; ‡MRI Institute, Department of Radiology, University of California, San Diego, Medical Center; §Moores Cancer Center, University of California, San Diego, La Jolla; ∥Departments of Medicine and Radiology, University of California, San Diego, Medical Center; and ¶Department of Chemistry and Biochemistry, University of California, San Diego, La Jolla.
Invest Radiol. 2014 Nov;49(11):707-19. doi: 10.1097/RLI.0000000000000074.
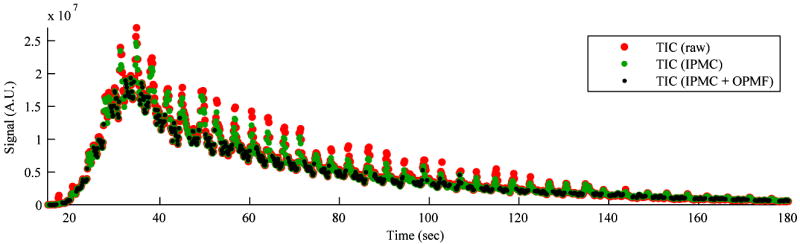
Contrast-enhanced ultrasound (CEUS) cines of focal liver lesions (FLLs) can be quantitatively analyzed to measure tumor perfusion on a pixel-by-pixel basis for diagnostic indication. However, CEUS cines acquired freehand and during free breathing cause nonuniform in-plane and out-of-plane motion from frame to frame. These motions create fluctuations in the time-intensity curves (TICs), reducing the accuracy of quantitative measurements. Out-of-plane motion cannot be corrected by image registration in 2-dimensional CEUS and degrades the quality of in-plane motion correction (IPMC). A 2-tier IPMC strategy and adaptive out-of-plane motion filter (OPMF) are proposed to provide a stable correction of nonuniform motion to reduce the impact of motion on quantitative analyses.
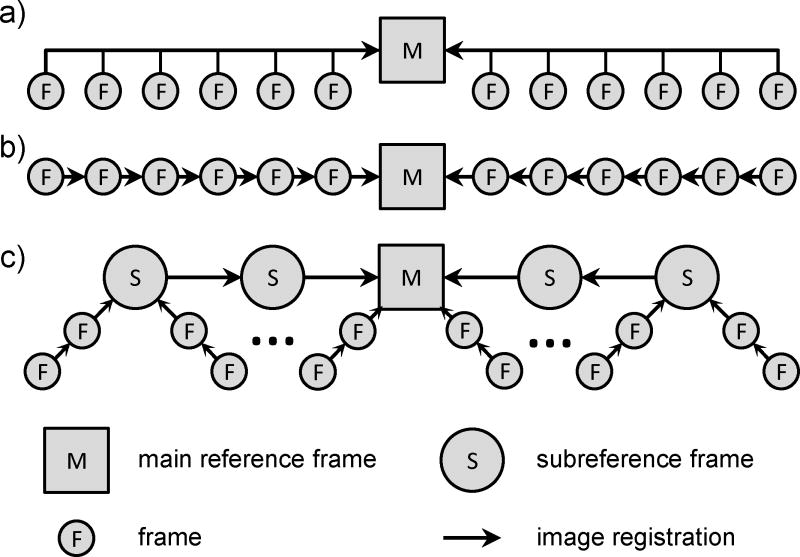
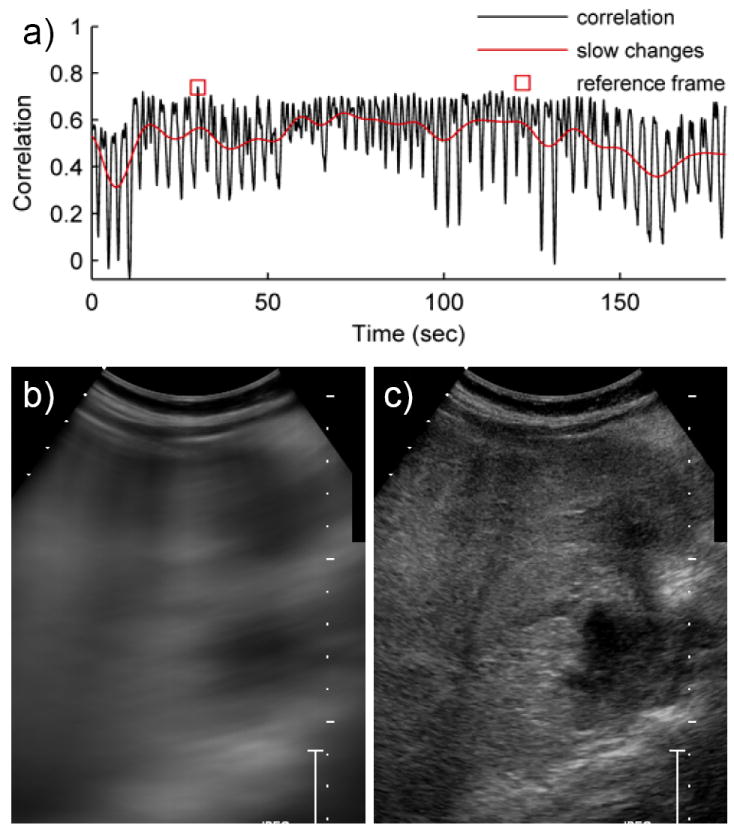
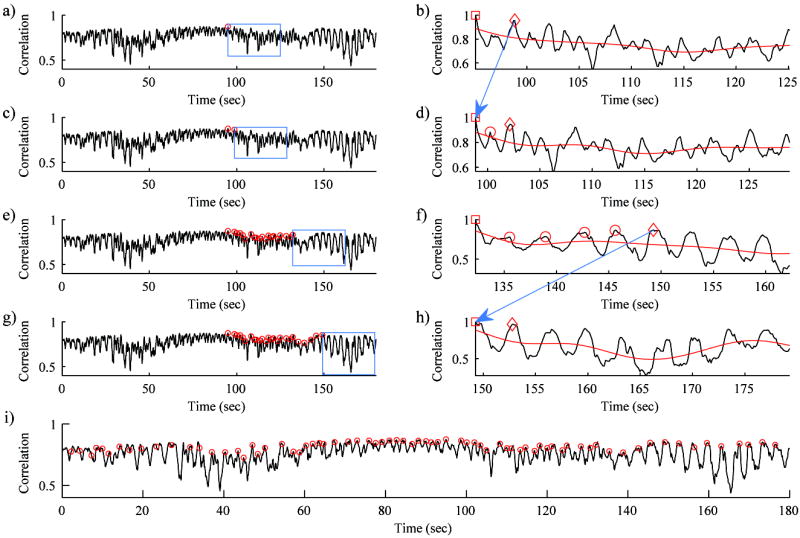
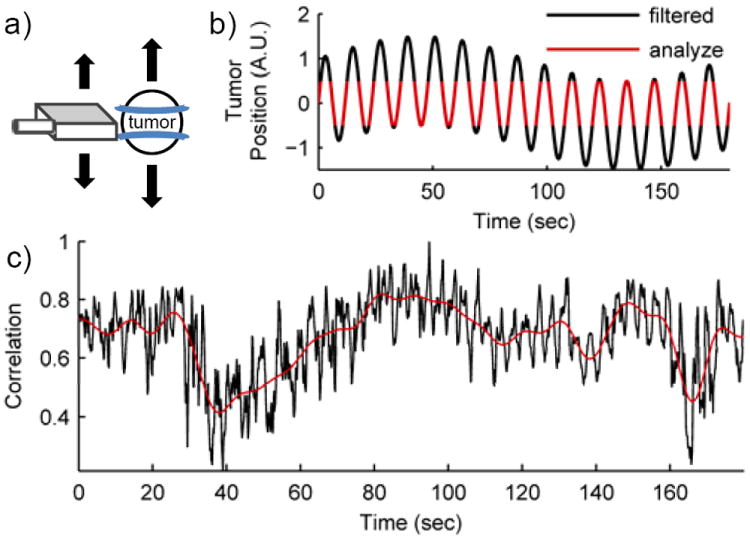
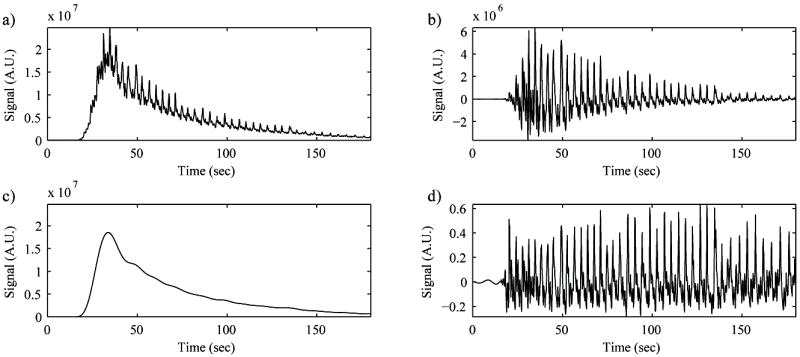
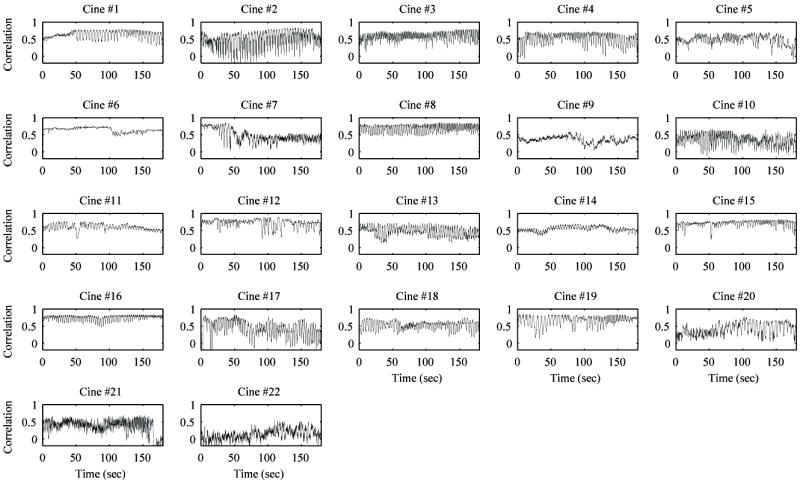
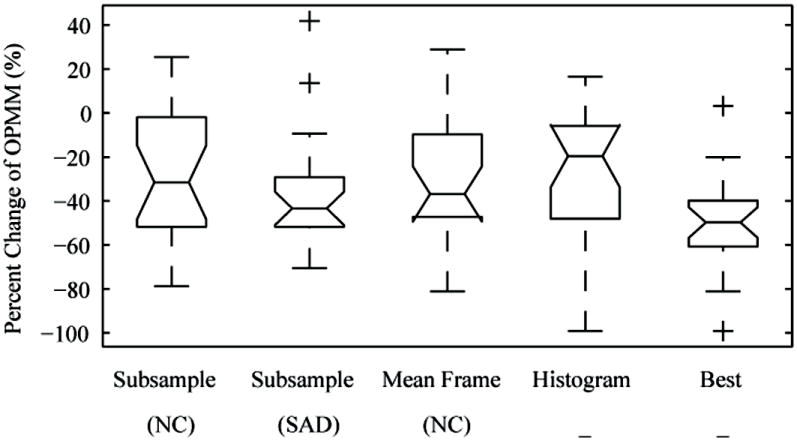
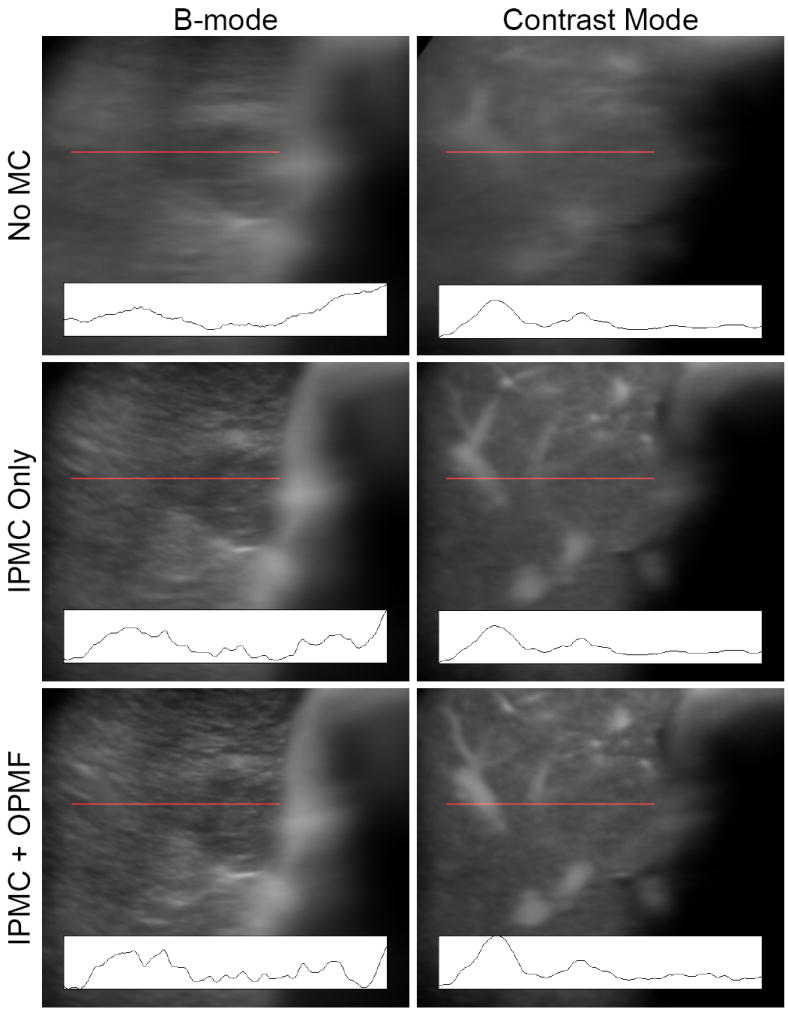
A total of 22 cines of FLLs were imaged with dual B-mode and contrast specific imaging to acquire a 3-minute TIC. B-mode images were analyzed for motion, and the motion correction was applied to both B-mode and contrast images. For IPMC, the main reference frame was automatically selected for each cine, and subreference frames were selected in each respiratory cycle and sequentially registered toward the main reference frame. All other frames were sequentially registered toward the local subreference frame. Four OPMFs were developed and tested: subsample normalized correlation (NC), subsample sum of absolute differences, mean frame NC, and histogram. The frames that were most dissimilar to the OPMF reference frame using 1 of the 4 above criteria in each respiratory cycle were adaptively removed by thresholding against the low-pass filter of the similarity curve. Out-of-plane motion filter was quantitatively evaluated by an out-of-plane motion metric (OPMM) that measured normalized variance in the high-pass filtered TIC within the tumor region-of-interest with low OPMM being the goal. Results for IPMC and OPMF were qualitatively evaluated by 2 blinded observers who ranked the motion in the cines before and after various combinations of motion correction steps.
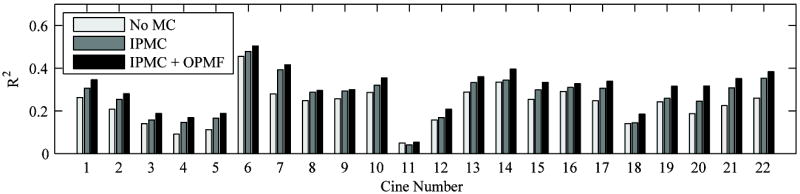
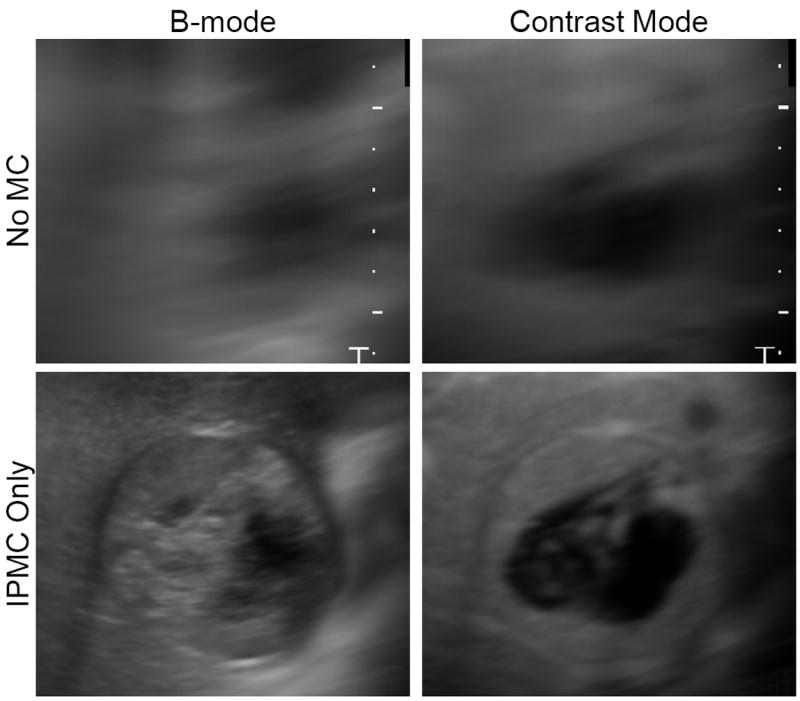
Quantitative measurements showed that 2-tier IPMC and OPMF improved imaging stability. With IPMC, the NC B-mode metric increased from 0.504 ± 0.149 to 0.585 ± 0.145 over all cines (P < 0.001). Two-tier IPMC also produced better fits on the contrast-specific TIC than industry standard IPMC techniques did (P < 0.02). In-plane motion correction and OPMF were shown to improve goodness of fit for pixel-by-pixel analysis (P < 0.001). Out-of-plane motion filter reduced variance in the contrast-specific signal as shown by a median decrease of 49.8% in the OPMM. Two-tier IPMC and OPMF were also shown to qualitatively reduce motion. Observers consistently ranked cines with IPMC higher than the same cine before IPMC (P < 0.001) as well as ranked cines with OPMF higher than when they were uncorrected.
The 2-tier sequential IPMC and adaptive OPMF significantly reduced motion in 3-minute CEUS cines of FLLs, thereby overcoming the challenges of drift and irregular breathing motion in long cines. The 2-tier IPMC strategy provided stable motion correction tolerant of out-of-plane motion throughout the cine by sequentially registering subreference frames that bypassed the motion cycles, thereby overcoming the lack of a nearly stationary reference point in long cines. Out-of-plane motion filter reduced apparent motion by adaptively removing frames imaged off-plane from the automatically selected OPMF reference frame, thereby tolerating nonuniform breathing motion. Selection of the best OPMF by minimizing OPMM effectively reduced motion under a wide variety of motion patterns applicable to clinical CEUS. These semiautomated processes only required user input for region-of-interest selection and can improve the accuracy of quantitative perfusion measurements.
可以对焦点性肝损伤(FLL)的超声造影(CEUS)电影进行定量分析,以逐像素测量肿瘤灌注用于诊断指征。然而,徒手获取以及在自由呼吸过程中获取的CEUS电影会导致帧间平面内和平面外运动不均匀。这些运动会在时间强度曲线(TIC)中产生波动,降低定量测量的准确性。二维CEUS中的图像配准无法校正平面外运动,并且会降低平面内运动校正(IPMC)的质量。本文提出了一种两级IPMC策略和自适应平面外运动滤波器(OPMF),以提供对不均匀运动的稳定校正,减少运动对定量分析的影响。
共对22个FLL的电影进行双B模式和造影剂特异性成像,以获取3分钟的TIC。分析B模式图像的运动情况,并将运动校正应用于B模式图像和造影剂图像。对于IPMC,为每个电影自动选择主参考帧,并在每个呼吸周期中选择子参考帧,并依次向主参考帧配准。所有其他帧依次向局部子参考帧配准。开发并测试了四种OPMF:子采样归一化互相关(NC)、子采样绝对差之和、平均帧NC和直方图。使用上述四种标准之一,在每个呼吸周期中与OPMF参考帧最不相似的帧,通过与相似性曲线的低通滤波器进行阈值比较来自适应去除。通过平面外运动度量(OPMM)对平面外运动滤波器进行定量评估,该度量测量肿瘤感兴趣区域内高通滤波TIC中的归一化方差,目标是使OPMM较低。由两名盲法观察者对IPMC和OPMF的结果进行定性评估,他们对各种运动校正步骤前后电影中的运动进行排名。
定量测量表明,两级IPMC和OPMF提高了成像稳定性。对于IPMC,所有电影的NC B模式度量从0.504±0.149增加到0.585±0.145(P<0.001)。两级IPMC在造影剂特异性TIC上的拟合也比行业标准IPMC技术更好(P<0.02)。平面内运动校正和OPMF被证明可以提高逐像素分析的拟合优度(P<0.001)。平面外运动滤波器降低了造影剂特异性信号的方差,如OPMM中位数下降49.8%所示。两级IPMC和OPMF在定性上也减少了运动。观察者一致将使用IPMC后的电影排名高于使用IPMC前的同一电影(P<0.001),并且将使用OPMF后的电影排名高于未校正时的电影。
两级顺序IPMC和自适应OPMF显著减少了FLL的3分钟CEUS电影中的运动,从而克服了长电影中漂移和不规则呼吸运动的挑战。两级IPMC策略通过依次配准绕过运动周期的子参考帧,提供了对整个电影平面外运动具有耐受性的稳定运动校正,从而克服了长电影中缺乏几乎静止参考点的问题。平面外运动滤波器通过从自动选择的OPMF参考帧中自适应去除平面外成像的帧来减少表观运动,从而耐受不均匀的呼吸运动。通过最小化OPMM选择最佳OPMF有效地减少了适用于临床CEUS的各种运动模式下的运动。这些半自动过程仅需要用户输入感兴趣区域的选择,并且可以提高定量灌注测量的准确性。