Sartipy Ulrik, Goda Ayumi, Mancini Donna M, Lund Lars H
Department of Cardiothoracic Surgery and Anesthesiology, Karolinska University Hospital, Stockholm, Sweden (U.S.) Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden (U.S.).
Cardiology Department, Kyorin University, Tokyo, Japan (A.G.).
J Am Heart Assoc. 2014 Jun 6;3(3):e000998. doi: 10.1161/JAHA.114.000998.
The 4-variable risk score from University of California, Los Angeles (UCLA) demonstrated superior discrimination in advanced heart failure, compared to established risk scores. However, the model has not been externally validated, and its suitability as a selection tool for heart transplantation (HT) and left ventricular assist device (LVAD) is unknown.
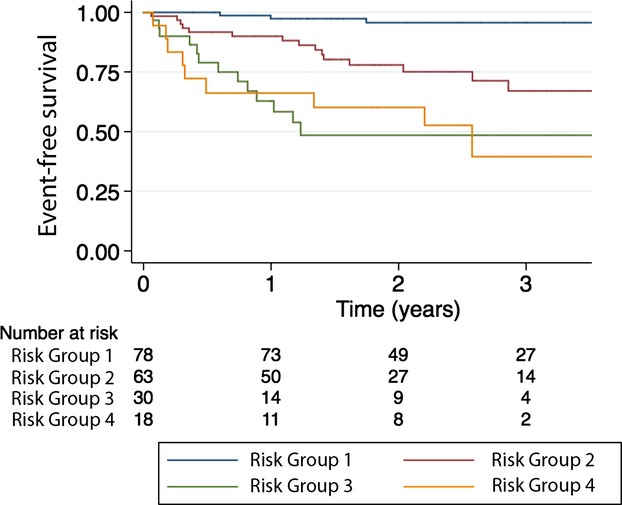
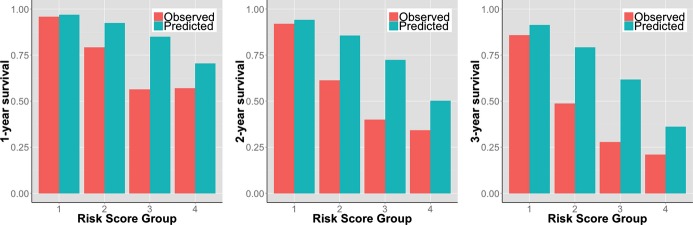
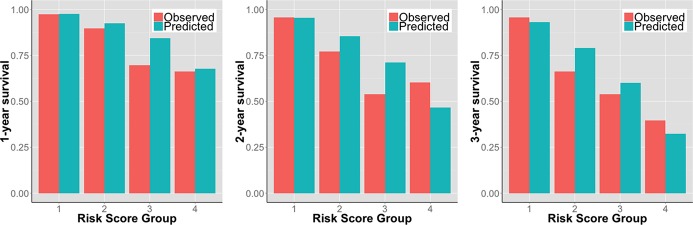
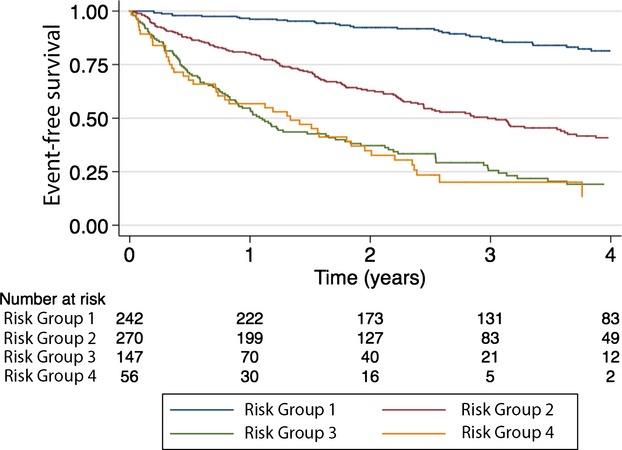
We calculated the UCLA risk score (based on B-type natriuretic peptide, peak VO2, New York Heart Association class, and use of angiotensin-converting enzyme inhibitor or angiotensin receptor blocker) in 180 patients referred for HT. The outcome was survival free from urgent transplantation or LVAD. The model-predicted survival was compared to Kaplan-Meier's estimated survival at 1, 2, and 3 years. Model discrimination and calibration were assessed. During a mean follow-up of 2.1 years, 37 (21%) events occurred. One-, 2- and 3-year observed event-free survival was 88%, 81%, and 75%, and the observed/predicted ratio was 0.97, 0.96, and 0.97, respectively. Time-dependent receiver operating characteristic curve analyses demonstrated good discrimination overall (1-year area under curve, 0.801; 2-year, 0.774; 3-year, 0.837), but discrimination between the 2 highest risk groups was poor. The difference between observed and predicted survival ranged from -14 to +17 percentage points, suggesting poor model calibration. Fairly similar results were found when the analyses were repeated in 715 patients after multivariate imputation of missing data.
The UCLA 4-variable risk model calibration was inconsistent and high-risk discrimination was poor in an external validation cohort. Further model assessment is warranted before widespread use.
与已有的风险评分相比,加利福尼亚大学洛杉矶分校(UCLA)的四变量风险评分在晚期心力衰竭中显示出更好的区分能力。然而,该模型尚未经过外部验证,其作为心脏移植(HT)和左心室辅助装置(LVAD)选择工具的适用性尚不清楚。
我们计算了180例接受HT评估患者的UCLA风险评分(基于B型利钠肽、峰值摄氧量、纽约心脏协会分级以及血管紧张素转换酶抑制剂或血管紧张素受体阻滞剂的使用情况)。结局为无紧急移植或LVAD植入的生存情况。将模型预测的生存率与Kaplan-Meier估计的1年、2年和3年生存率进行比较。评估模型的区分能力和校准情况。在平均2.1年的随访期间,发生了37例(21%)事件。1年、2年和3年观察到的无事件生存率分别为88%、81%和75%,观察值/预测值分别为0.97、0.96和0.97。时间依赖性受试者工作特征曲线分析总体显示出良好的区分能力(1年曲线下面积为0.801;2年为0.774;3年为0.837),但两个最高风险组之间的区分能力较差。观察到的和预测的生存率之间的差异在-14至+17个百分点之间,表明模型校准较差。在对缺失数据进行多变量插补后,对715例患者重复进行分析时发现了相当相似的结果。
在外部验证队列中,UCLA四变量风险模型校准不一致,高风险区分能力较差。在广泛应用之前,有必要进一步评估该模型。