Mohri Yasuhiko, Tanaka Koji, Ohi Masaki, Saigusa Susumu, Yasuda Hiromi, Toiyama Yuji, Araki Toshimitu, Inoue Yasuhiro, Kusunoki Masato
Department of Gastrointestinal and Pediatric Surgery, Mie University Graduate School of Medicine, Tsu, Japan.
BMC Cancer. 2014 Jun 6;14:409. doi: 10.1186/1471-2407-14-409.
The treatment of metastatic gastric cancer is not uniform, and the prognostic factors and indications for surgery are currently unclear. This retrospective study aimed to identify the prognostic factors and clinical indications for surgery in patients with metastatic gastric cancer.
A total of 123 consecutive patients with gastric cancer and synchronous distant metastasis treated between January 1999 and December 2011 were reviewed. Patient, tumor, laboratory, surgical, and chemotherapy factors were analyzed, with overall survival as the endpoint. Univariate analyses were performed using the log-rank test, multivariate analyses were performed using the Cox proportional hazards model, and Kaplan-Meier curves were used to estimate survival. Significance was set at p<0.05.
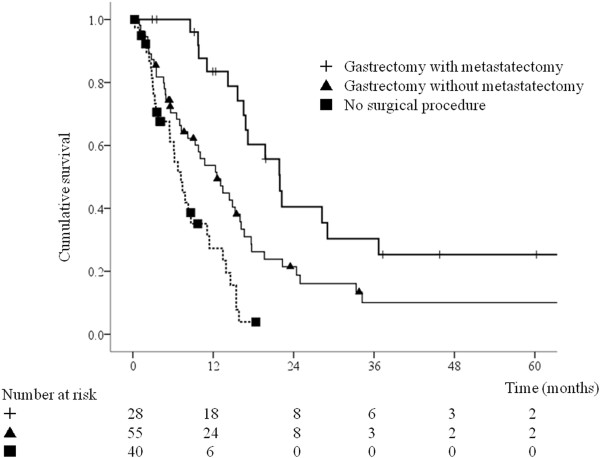
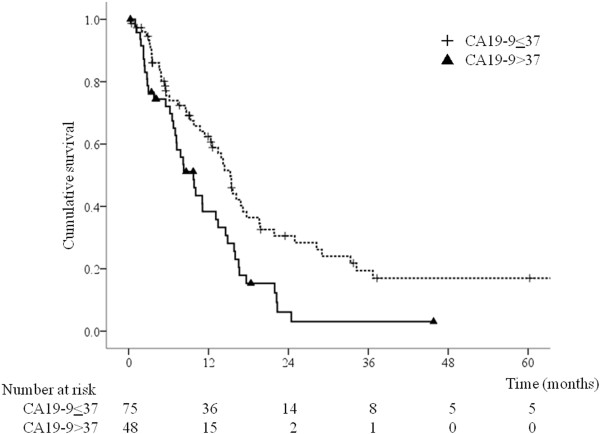
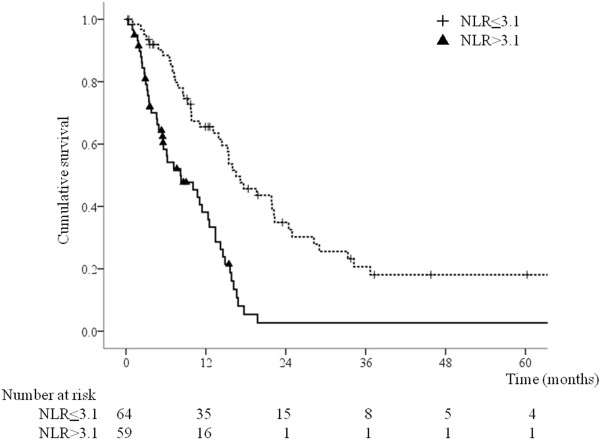
The median overall survival time was 13.1 months. Ninety-eight patients received chemotherapy. Twenty-eight patients underwent gastrectomy with metastasectomy and 55 underwent gastrectomy without metastasectomy. The median overall survival time for patients who underwent gastrectomy with metastasectomy, gastrectomy without metastasectomy, and no surgical intervention was 21.9 months, 12.5 months, and 7.2 months, respectively (p<0.001). Multivariate analysis identified gastrectomy with or without metastasectomy, performance status (PS) ≥ 3, neutrophil-to-lymphocyte ratio (NLR) >3.1, and carbohydrate antigen 19-9 (CA19-9) level >37 U/mL as predictors of poor survival. NLR and CA19-9 level were also independent prognostic factors in the group of patients who underwent surgery.
High pretreatment NLR, CA19-9 level, and PS are predictors of poor prognosis in patients with metastatic gastric cancer. In selected patients, gastrectomy can be performed safely, and may be associated with longer survival.
转移性胃癌的治疗方法并不统一,目前其预后因素和手术指征尚不清楚。这项回顾性研究旨在确定转移性胃癌患者的预后因素和手术的临床指征。
回顾了1999年1月至2011年12月期间连续治疗的123例患有胃癌并伴有同步远处转移的患者。分析了患者、肿瘤、实验室、手术和化疗因素,以总生存期作为终点。使用对数秩检验进行单因素分析,使用Cox比例风险模型进行多因素分析,并使用Kaplan-Meier曲线估计生存率。显著性设定为p<0.05。
中位总生存时间为13.1个月。98例患者接受了化疗。28例患者接受了胃切除术并切除转移灶,55例患者接受了胃切除术但未切除转移灶。接受胃切除术并切除转移灶、胃切除术但未切除转移灶以及未进行手术干预的患者的中位总生存时间分别为21.9个月、12.5个月和7.2个月(p<0.001)。多因素分析确定,无论是否切除转移灶的胃切除术、体能状态(PS)≥3、中性粒细胞与淋巴细胞比值(NLR)>3.1以及糖类抗原19-9(CA19-9)水平>37 U/mL是生存不良的预测因素。NLR和CA19-9水平也是接受手术患者组的独立预后因素。
治疗前高NLR、CA19-9水平和PS是转移性胃癌患者预后不良的预测因素。在选定的患者中,可以安全地进行胃切除术,并且可能与更长的生存期相关。