Koreth John, Kim Haesook T, Nikiforow Sarah, Milford Edgar L, Armand Philippe, Cutler Corey, Glotzbecker Brett, Ho Vincent T, Antin Joseph H, Soiffer Robert J, Ritz Jerome, Alyea Edwin P
Hematologic Malignancies Division, Dana-Farber Cancer Institute, Boston, Massachusetts.
Division of Biostatistics and Computational Biology, Dana-Farber Cancer Institute, Boston, Massachusetts.
Biol Blood Marrow Transplant. 2014 Oct;20(10):1516-21. doi: 10.1016/j.bbmt.2014.05.025. Epub 2014 Jun 4.
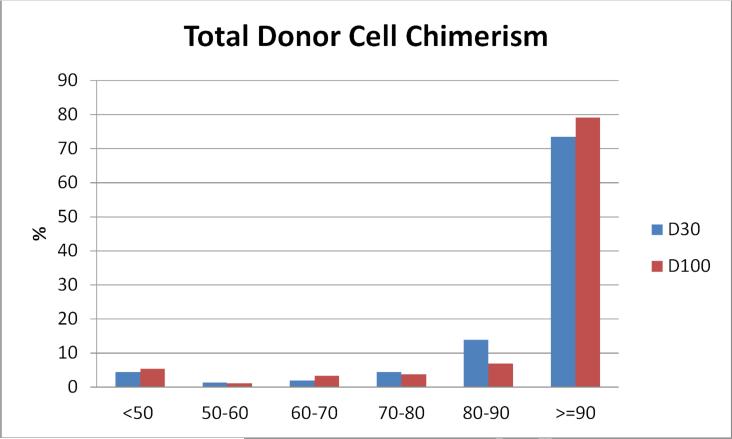
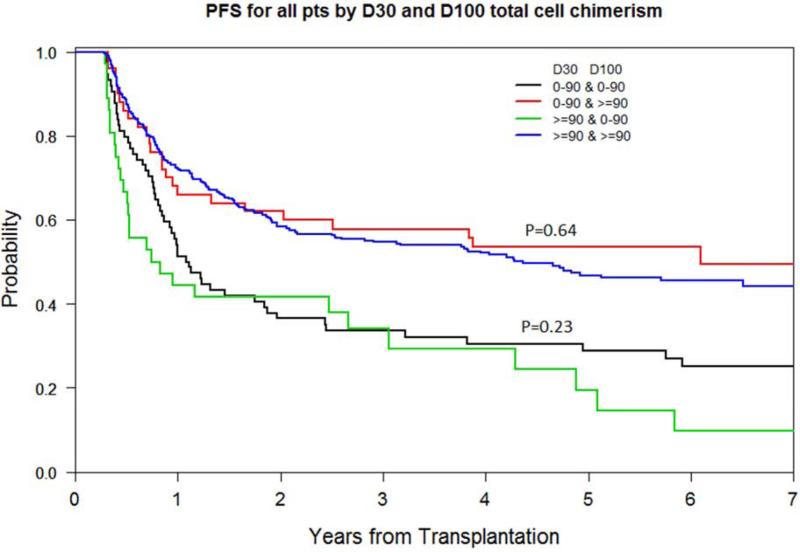
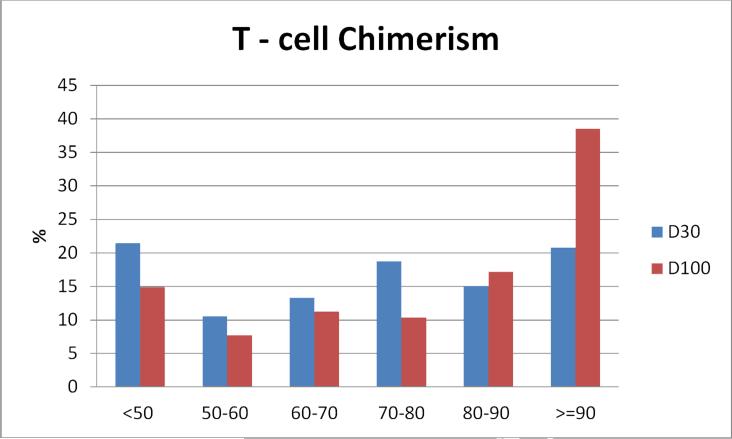
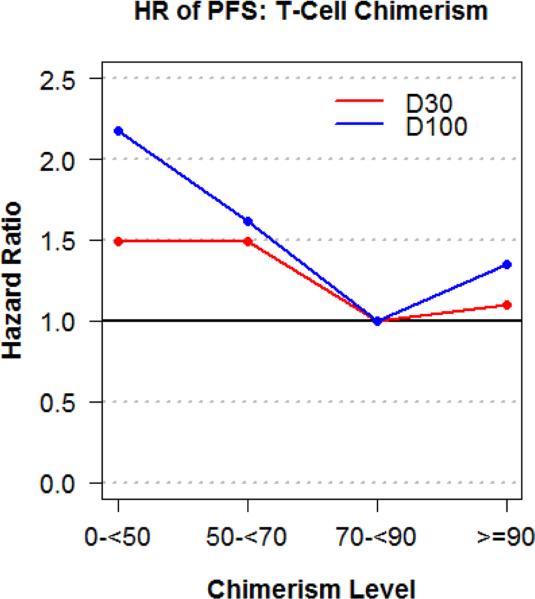
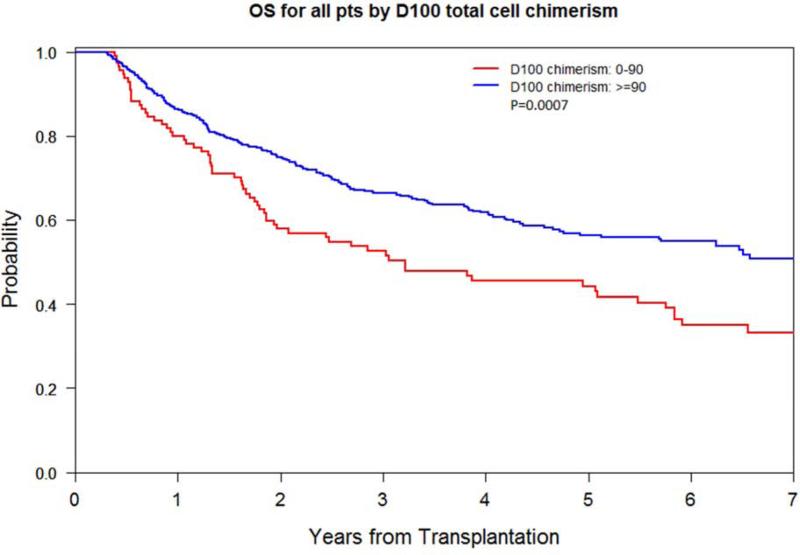
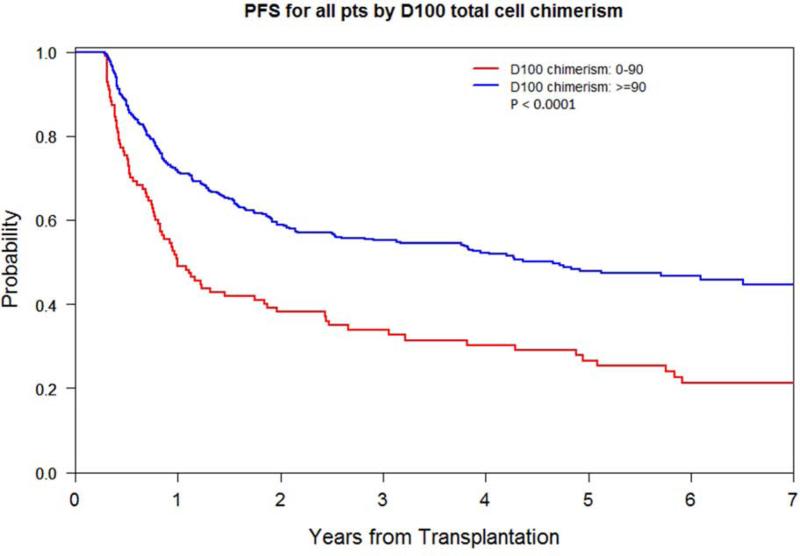
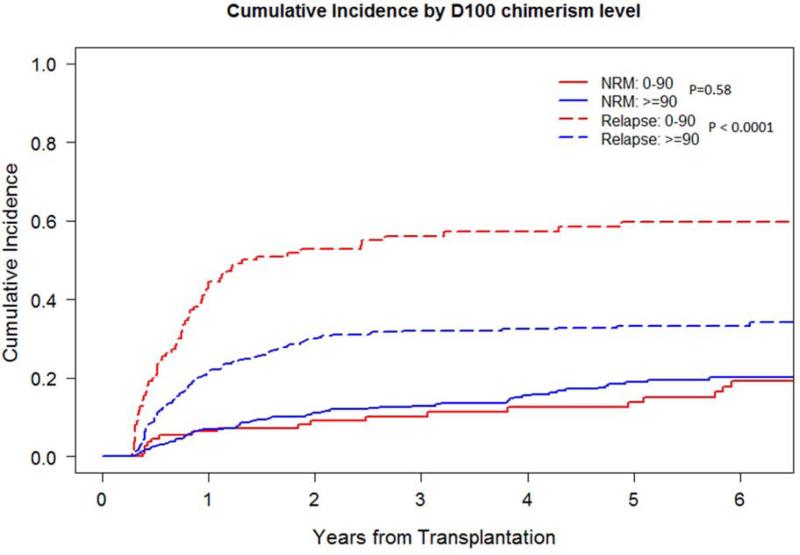
The impact of early donor cell chimerism on outcomes of T cell-replete reduced-intensity conditioning (RIC) hematopoietic stem cell transplantation (HSCT) is ill defined. We evaluated day 30 (D30) and 100 (D100) total donor cell chimerism after RIC HSCT undertaken between 2002 and 2010 at our institution, excluding patients who died or relapsed before D30. When available, donor T cell chimerism was also assessed. The primary outcome was overall survival (OS). Secondary outcomes included progression-free survival (PFS), relapse, and nonrelapse mortality (NRM). We evaluated 688 patients with hematologic malignancies (48% myeloid and 52% lymphoid) and a median age of 57 years (range, 18 to 74) undergoing RIC HSCT with T cell-replete donor grafts (97% peripheral blood; 92% HLA-matched), with a median follow-up of 58.2 months (range, 12.6 to 120.7). In multivariable analysis, total donor cell and T cell chimerism at D30 and D100 each predicted RIC HSCT outcomes, with D100 total donor cell chimerism most predictive. D100 total donor cell chimerism <90% was associated with increased relapse (hazard ratio [HR], 2.54; 95% confidence interval [CI], 1.83 to 3.51; P < .0001), impaired PFS (HR, 2.01; 95% CI, 1.53 to 2.65; P < .0001), and worse OS (HR, 1.50; 95% CI, 1.11 to 2.04, P = .009), but not with NRM (HR, .76; 95% CI, .44 to 2.27; P = .33). There was no additional utility of incorporating sustained D30 to D100 total donor cell chimerism or T cell chimerism. Low donor chimerism early after RIC HSCT is an independent risk factor for relapse and impaired survival. Donor chimerism assessment early after RIC HSCT can prognosticate for long-term outcomes and help identify high-risk patient cohorts who may benefit from additional therapeutic interventions.
早期供体细胞嵌合现象对T细胞充足的低强度预处理(RIC)造血干细胞移植(HSCT)结果的影响尚不明确。我们评估了2002年至2010年在我们机构进行RIC HSCT后第30天(D30)和第100天(D100)的总供体细胞嵌合率,排除了在D30之前死亡或复发的患者。如有可能,还评估了供体T细胞嵌合率。主要结局是总生存期(OS)。次要结局包括无进展生存期(PFS)、复发和非复发死亡率(NRM)。我们评估了688例血液系统恶性肿瘤患者(48%为髓系,52%为淋巴系),中位年龄57岁(范围18至74岁),接受了T细胞充足的供体移植物(97%为外周血;92%为HLA匹配)的RIC HSCT,中位随访时间为58.2个月(范围12.6至120.7个月)。在多变量分析中,D30和D100时的总供体细胞和T细胞嵌合率均预测了RIC HSCT的结果,其中D100时的总供体细胞嵌合率预测性最强。D100时总供体细胞嵌合率<90%与复发增加(风险比[HR],2.54;95%置信区间[CI],1.83至3.51;P <.0001)、PFS受损(HR,2.01;95% CI,1.53至2.65;P <.0001)和OS较差(HR,1.50;95% CI,1.11至2.04,P =.009)相关,但与NRM无关(HR,.76;95% CI,.44至2.27;P =.33)。纳入D30至D100持续的总供体细胞嵌合率或T细胞嵌合率并无额外益处。RIC HSCT后早期供体嵌合率低是复发和生存受损的独立危险因素。RIC HSCT后早期评估供体嵌合率可预测长期结局,并有助于识别可能从额外治疗干预中获益的高危患者队列。