Cardno ChemRisk, LLC Aliso Viejo, CA, USA.
ToxStrategies Tallahassee, FL, USA.
Front Genet. 2014 May 30;5:151. doi: 10.3389/fgene.2014.00151. eCollection 2014.
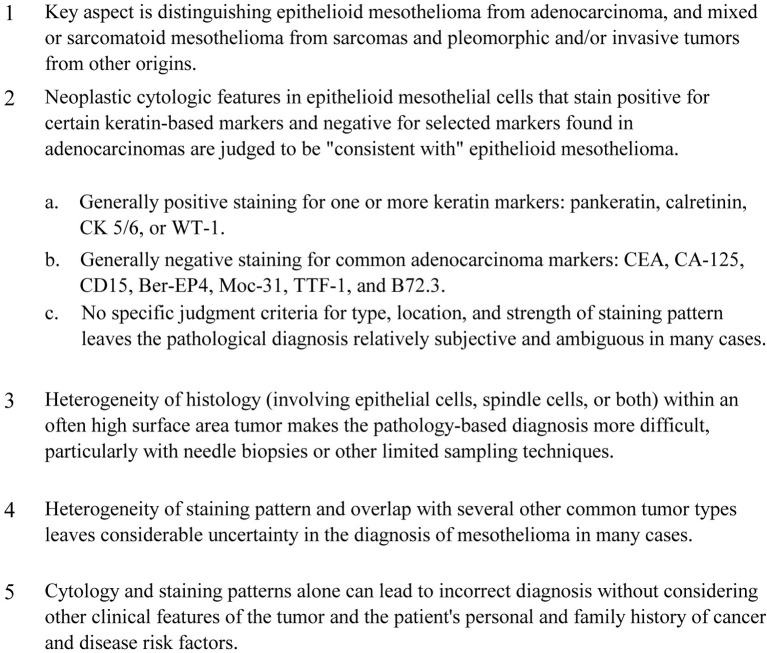
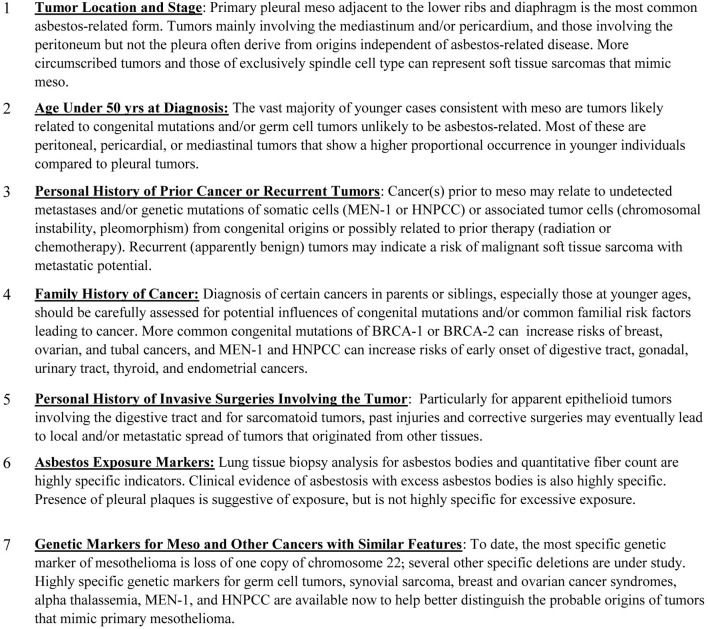
The diagnosis of mesothelioma is not always straightforward, despite known immunohistochemical markers and other diagnostic techniques. One reason for the difficulty is that extrapleural tumors resembling mesothelioma may have several possible etiologies, especially in cases with no meaningful history of amphibole asbestos exposure. When the diagnosis of mesothelioma is based on histologic features alone, primary mesotheliomas may resemble various primary or metastatic cancers that have directly invaded the serosal membranes. Some of these metastatic malignancies, particularly carcinomas and sarcomas of the pleura, pericardium and peritoneum, may undergo desmoplastic reaction in the pleura, thereby mimicking mesothelioma, rather than the primary tumor. Encasement of the lung by direct spread or metastasis, termed pseudomesotheliomatous spread, occurs with several other primary cancer types, including certain late-stage tumors from genetic cancer syndromes exhibiting chromosomal instability. Although immunohistochemical staining patterns differentiate most carcinomas, lymphomas, and mestastatic sarcomas from mesotheliomas, specific genetic markers in tumor or somatic tissues have been recently identified that may also distinguish these tumor types from asbestos-related mesothelioma. A registry for genetic screening of mesothelioma cases would help lead to improvements in diagnostic criteria, prognostic accuracy and treatment efficacy, as well as improved estimates of primary mesothelioma incidence and of background rates of cancers unrelated to asbestos that might be otherwise mistaken for mesothelioma. This information would also help better define the dose-response relationships for mesothelioma and asbestos exposure, as well as other risk factors for mesothelioma and other mesenchymal or advanced metastatic tumors that may be indistinguishable by histology and staining characteristics.
尽管有已知的免疫组织化学标志物和其他诊断技术,但间皮瘤的诊断并不总是那么简单。造成这种困难的原因之一是,与间皮瘤相似的胸膜外肿瘤可能有几种可能的病因,尤其是在没有石棉暴露史的情况下。当间皮瘤的诊断仅基于组织学特征时,原发性间皮瘤可能类似于直接侵犯浆膜的各种原发性或转移性癌症。这些转移性恶性肿瘤中的一些,特别是胸膜、心包和腹膜的癌和肉瘤,可能在胸膜发生纤维母细胞反应,从而模仿间皮瘤,而不是原发性肿瘤。肺的直接扩散或转移导致的肺包裹,称为假间皮瘤样扩散,发生在几种其他原发性癌症类型中,包括某些具有染色体不稳定性的遗传性癌症综合征的晚期肿瘤。虽然免疫组织化学染色模式可区分大多数癌、淋巴瘤和转移性肉瘤与间皮瘤,但最近在肿瘤或体细胞组织中发现了特定的遗传标记,也可能将这些肿瘤类型与石棉相关的间皮瘤区分开来。间皮瘤病例的遗传筛查登记将有助于改进诊断标准、预后准确性和治疗效果,以及改善与石棉无关的原发性间皮瘤发病率和可能被误诊为间皮瘤的癌症的背景率的估计。这些信息还将有助于更好地定义间皮瘤与石棉暴露的剂量反应关系,以及间皮瘤和其他间充质或晚期转移性肿瘤的其他危险因素,这些肿瘤在组织学和染色特征上可能无法区分。