Clemens Andreas, Noack Herbert, Brueckmann Martina, Lip Gregory Y H
Center for Thrombosis and Hemostasis (CTH), University Medical Center Mainz, Mainz, Germany; Global Biostatistics and Data Management, Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim, Germany.
Corporate Division Medicine, Global Therapeutic Area Cardiovascular, Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim, Germany.
PLoS One. 2014 Jun 9;9(6):e99276. doi: 10.1371/journal.pone.0099276. eCollection 2014.
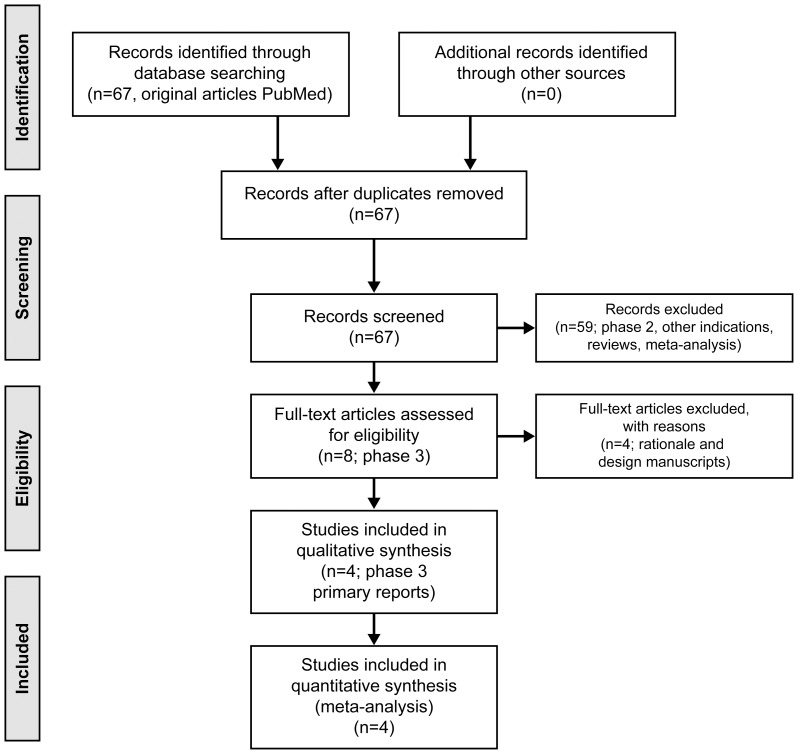
A number of novel oral anticoagulants (direct thrombin inhibitors or factor Xa inhibitors) are in clinical use for various indications. The dosing regimens differ between twice-daily and once-daily dosing for the prevention of stroke in patients with atrial fibrillation. With the availability of the results from four phase 3 studies (>70,000 patients), we explored whether twice-daily or once-daily dosing provides better risk-benefit balance among novel oral anticoagulants.
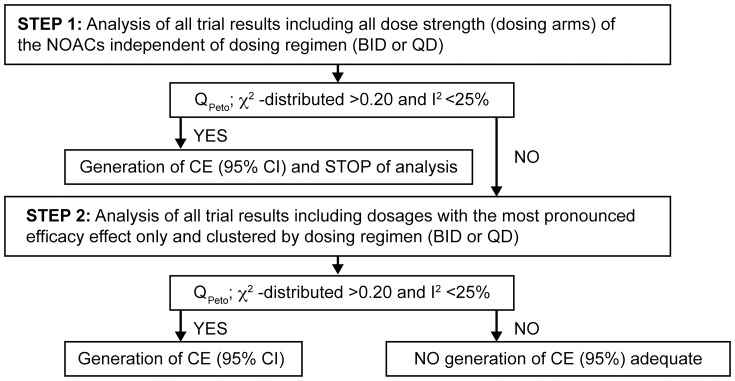
We conducted a strict, stepwise, fixed-effects meta-analysis with predefined heterogeneity quality criteria to generate the most appropriate common estimates for twice-daily (BID) or once-daily (QD) dosing regimens. An indirect comparison of these dosing regimens with fixed-effects meta-analysis common estimates (where available), or individual compound results, was done respectively.
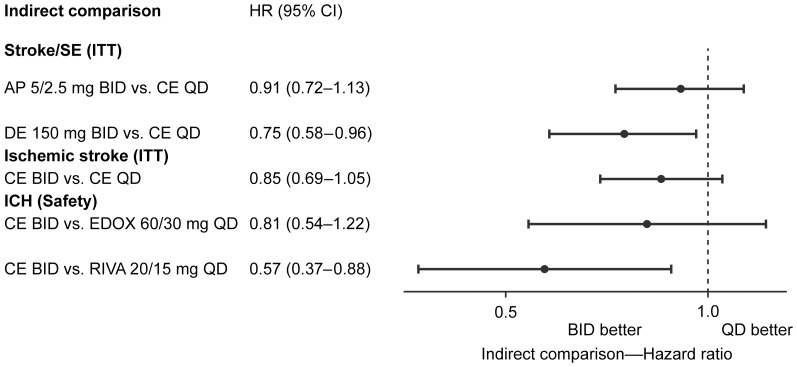
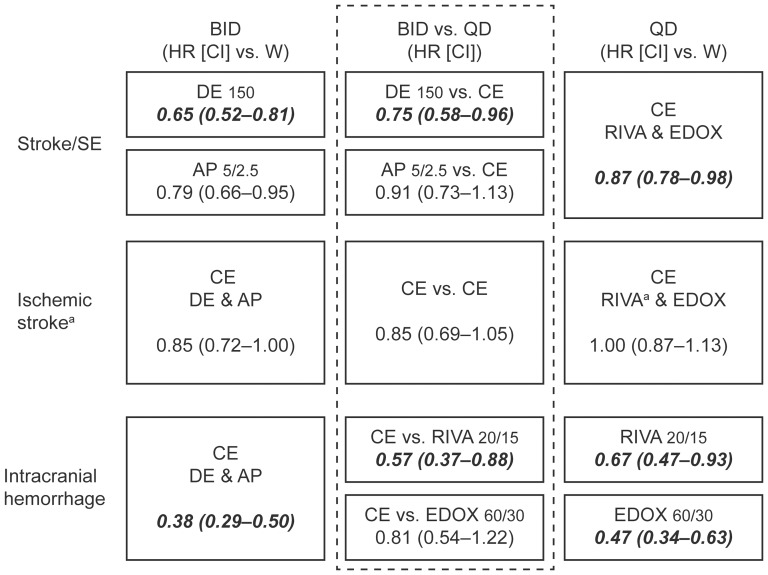
Comparing indirectly BID vs QD dosing regimens resulted in hazard ratios (HR [95% confidence interval]) for stroke and systemic embolism of 0.75 (0.58-0.96) for dabigatran 150 mg BID, and 0.91 (0.73-1.13) for apixaban BID vs the QD dosing regimen. For ischemic stroke, the HR of BID vs QD was 0.85 (0.69-1.05). For intracranial hemorrhage, BID vs rivaroxaban QD was 0.57 (0.37-0.88) and, vs edoxaban QD, 0.81 (0.54-1.22). Due to heterogeneity, common estimates for major bleeding QD or BID were not justified, therefore indirect comparison of regimens were not possible. All non-vitamin K antagonist oral anticoagulants reduced all-cause mortality vs warfarin with a HR of 0.90 (0.86-0.96) without differences between regimen.
Based on the available phase 3 study evidence, the twice-daily dosing regimen of non-vitamin K antagonist oral anticoagulants appears to offer a more balanced risk-benefit profile with respect to stroke prevention and intracranial hemorrhage.
多种新型口服抗凝剂(直接凝血酶抑制剂或Xa因子抑制剂)已在临床上用于多种适应症。在预防心房颤动患者中风方面,每日两次给药方案与每日一次给药方案不同。随着四项3期研究(超过70000名患者)结果的公布,我们探讨了在新型口服抗凝剂中,每日两次给药还是每日一次给药能提供更好的风险效益平衡。
我们进行了一项严格的、逐步的固定效应荟萃分析,采用预定义的异质性质量标准,以得出每日两次(BID)或每日一次(QD)给药方案最合适的共同估计值。分别对这些给药方案与固定效应荟萃分析共同估计值(如可用)或单个化合物结果进行间接比较。
间接比较每日两次与每日一次给药方案,达比加群150mg每日两次方案的中风和全身性栓塞的风险比(HR[95%置信区间])为0.75(0.58 - 0.96),阿哌沙班每日两次方案与每日一次给药方案相比的风险比为0.91(0.73 - 1.13)。对于缺血性中风,每日两次与每日一次的HR为0.85(0.69 - 1.05)。对于颅内出血,每日两次与利伐沙班每日一次相比为0.57(0.37 - 0.88),与依度沙班每日一次相比为0.81(0.54 - 1.22)。由于存在异质性,每日一次或每日两次主要出血的共同估计值不合理,因此无法对给药方案进行间接比较。所有非维生素K拮抗剂口服抗凝剂与华法林相比均降低了全因死亡率,HR为0.90(0.86 - 0.96),不同给药方案之间无差异。
基于现有的3期研究证据,非维生素K拮抗剂口服抗凝剂的每日两次给药方案在预防中风和颅内出血方面似乎提供了更平衡的风险效益概况。