Sun Yu-Yo, Morozov Yury M, Yang Dianer, Li Yikun, Dunn R Scott, Rakic Pasko, Chan Pak H, Abe Koji, Lindquist Diana M, Kuan Chia-Yi
Department of Pediatrics, Emory University School of Medicine and Children's Healthcare of Atlanta, Atlanta, Georgia, United States of America.
Department of Neurobiology, Yale University School of Medicine, New Haven, Connecticut, United States of America.
PLoS One. 2014 Jun 9;9(6):e98807. doi: 10.1371/journal.pone.0098807. eCollection 2014.
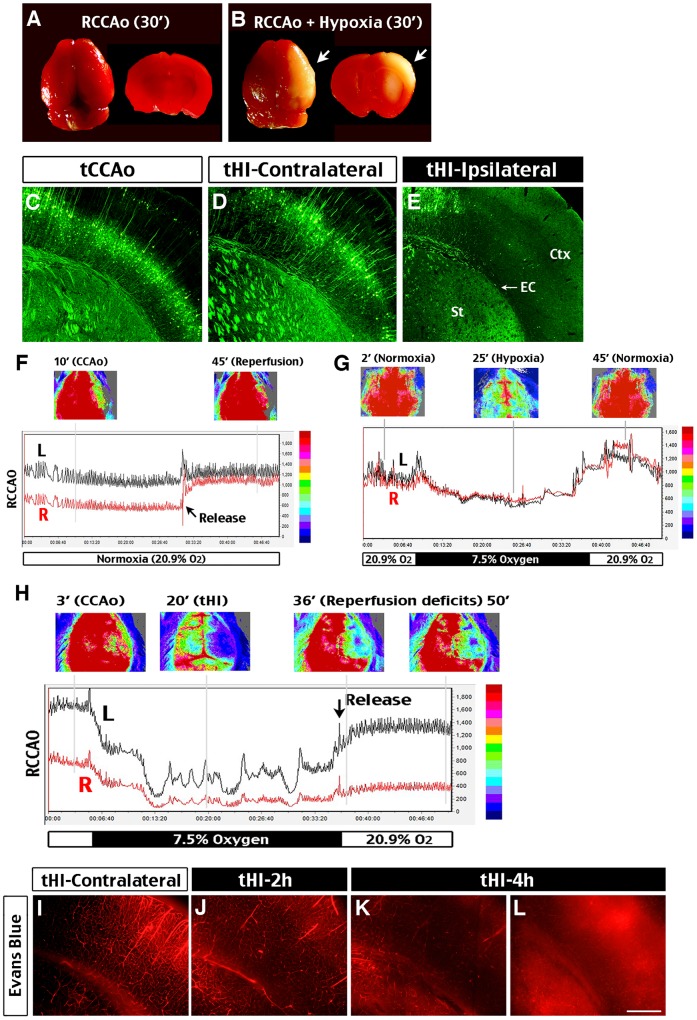
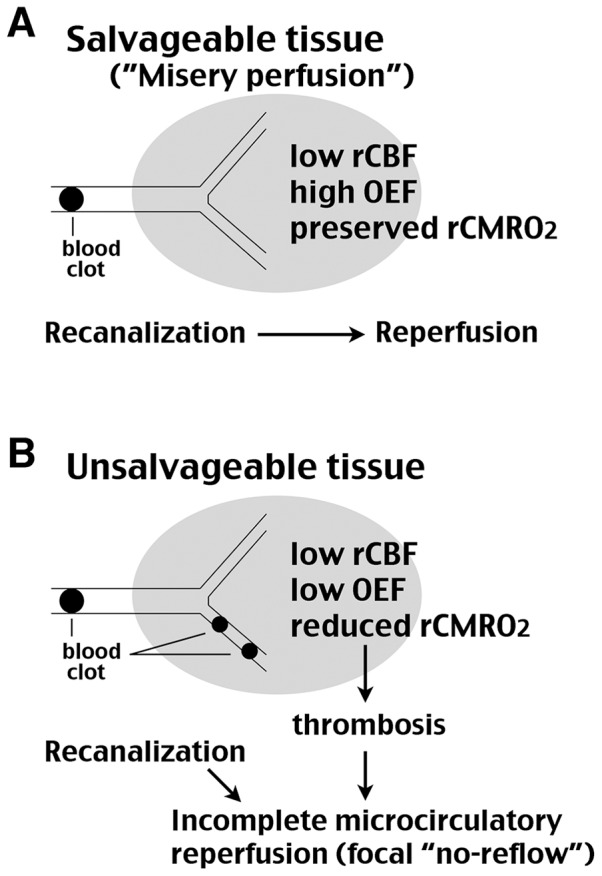
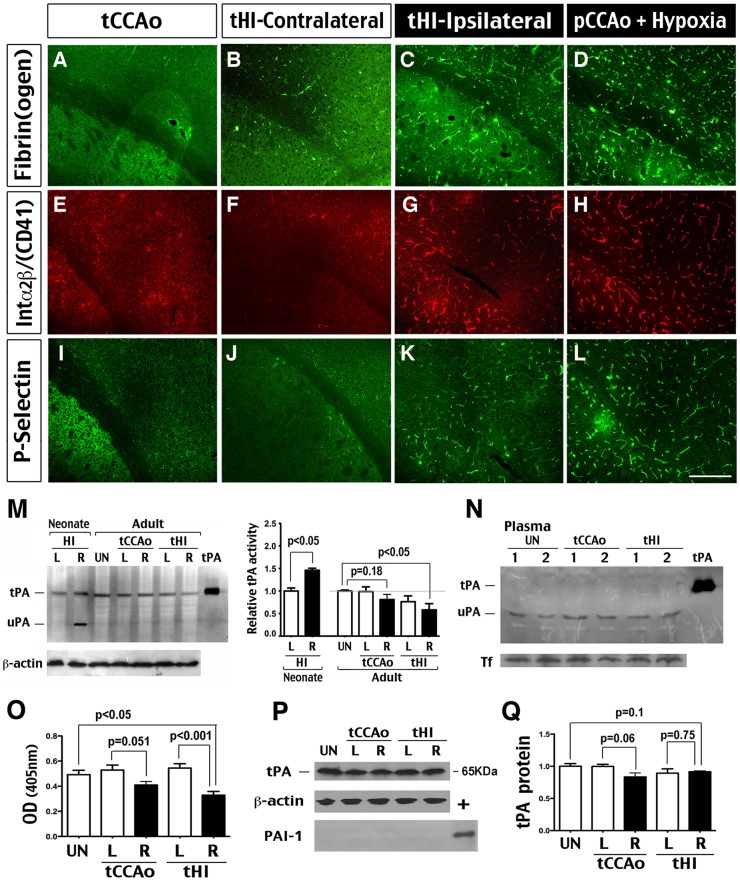
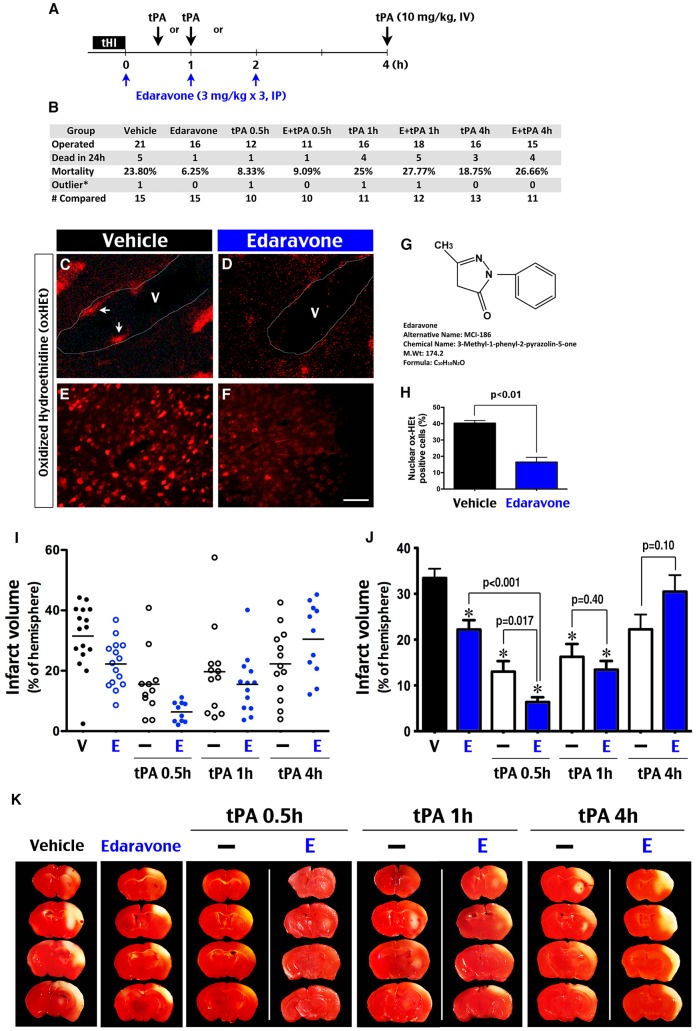
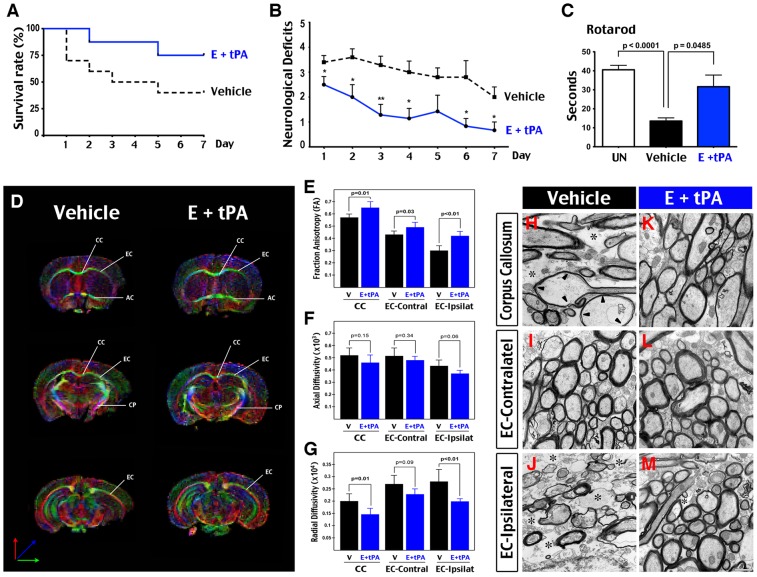
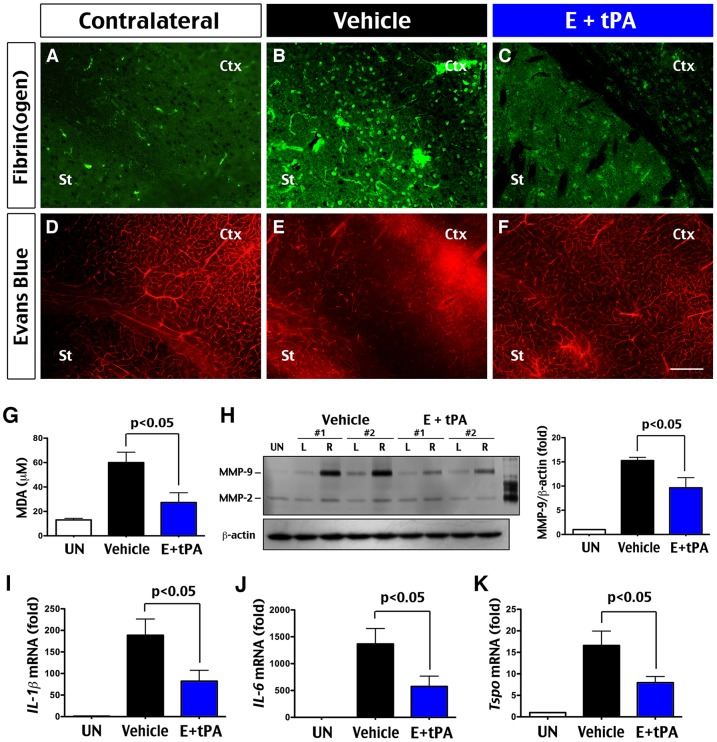
Edaravone, a potent antioxidant, may improve thrombolytic therapy because it benefits ischemic stroke patients on its own and mitigates adverse effects of tissue plasminogen activator (tPA) in preclinical models. However, whether the combined tPA-edaravone therapy is more effective in reducing infarct size than singular treatment is uncertain. Here we investigated this issue using a transient hypoxia-ischemia (tHI)-induced thrombotic stroke model, in which adult C57BL/6 mice were subjected to reversible ligation of the unilateral common carotid artery plus inhalation of 7.5% oxygen for 30 min. While unilateral occlusion of the common carotid artery suppressed cerebral blood flow transiently, the addition of hypoxia triggered reperfusion deficits, endogenous thrombosis, and attenuated tPA activity, leading up to infarction. We compared the outcomes of vehicle-controls, edaravone treatment, tPA treatment at 0.5, 1, or 4 h post-tHI, and combined tPA-edaravone therapies with mortality rate and infarct size as the primary end-points. The best treatment was further compared with vehicle-controls in behavioral, biochemical, and diffusion tensor imaging (DTI) analyses. We found that application of tPA at 0.5 or 1 h--but not at 4 h post-tHI--significantly decreased infarct size and showed synergistic (p<0.05) or additive benefits with the adjuvant edaravone treatment, respectively. The acute tPA-edaravone treatment conferred >50% reduction of mortality, ∼ 80% decline in infarct size, and strong white-matter protection. It also improved vascular reperfusion and decreased oxidative stress, inflammatory cytokines, and matrix metalloproteinase activities. In conclusion, edaravone synergizes with acute tPA treatment in experimental thrombotic stroke, suggesting that clinical application of the combined tPA-edaravone therapy merits investigation.
依达拉奉是一种强效抗氧化剂,可能会改善溶栓治疗,因为它本身对缺血性中风患者有益,并且在临床前模型中可减轻组织纤溶酶原激活剂(tPA)的不良反应。然而,tPA与依达拉奉联合治疗在减小梗死面积方面是否比单一治疗更有效尚不确定。在此,我们使用短暂缺氧缺血(tHI)诱导的血栓性中风模型研究了这个问题,在该模型中,成年C57BL/6小鼠接受单侧颈总动脉可逆性结扎并吸入7.5%氧气30分钟。虽然单侧颈总动脉闭塞会短暂抑制脑血流量,但缺氧会引发再灌注缺陷、内源性血栓形成并减弱tPA活性,最终导致梗死。我们以死亡率和梗死面积作为主要终点,比较了溶媒对照组、依达拉奉治疗组、tHI后0.5、1或4小时的tPA治疗组以及tPA与依达拉奉联合治疗组的结果。在行为、生化和扩散张量成像(DTI)分析中,将最佳治疗组与溶媒对照组进一步进行了比较。我们发现,在tHI后0.5或1小时应用tPA(而非4小时)可显著减小梗死面积,并且分别与辅助性依达拉奉治疗显示出协同(p<0.05)或相加益处。急性tPA与依达拉奉联合治疗可使死亡率降低>50%,梗死面积减少约80%,并对白质有强大的保护作用。它还改善了血管再灌注,降低了氧化应激、炎性细胞因子和基质金属蛋白酶活性。总之,依达拉奉与急性tPA治疗在实验性血栓性中风中具有协同作用,这表明tPA与依达拉奉联合治疗的临床应用值得研究。