Pasticci Maria Bruna, Di Filippo Paolo, Pasqualini Leonella, Mencacci Antonella, Pallotto Carlo, Malincarne Lisa, Baldelli Franco
Infectious Disease Section, Department of Experimental Medicine and Biochemical Sciences, University of Perugia, 06100 Perugia, Italy.
J Med Case Rep. 2014 Jun 12;8:186. doi: 10.1186/1752-1947-8-186.
Prosthetic joint infections are severe complications of joint implants. Further complications arise when polymicrobial and/or multidrug-resistant microorganisms are involved. Currently, there are limited data on the management of these infections and on the tolerability of long-term treatment with daptomycin, ceftazidime and colistin.
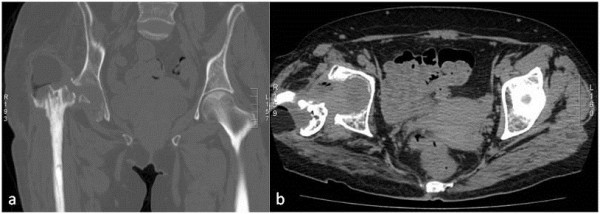
A 55-year-old Caucasian woman who had a right hip prosthesis removed 1 year prior because of infection was admitted for prosthesis reimplantation. On admission at our hospital, anamnesis regarding etiology and management of prosthesis infection was not available. On clinical, laboratory findings and imaging studies infection was not suspected. A hip prosthesis was reimplanted. At surgery, histopathological and microbiological investigations were not taken. Three weeks after reimplantation, surgical site infection due to Enterobacter cloacae was diagnosed and oral ciprofloxacin was prescribed. Four days later, a periprosthesis fluid collection was evidenced and a percutaneous needle aspirate grew Staphylococcus epidermidis and S. haemolyticus. Enterobacter genome was also detected from the same sample. Teicoplanin and meropenem were added to ciprofloxacin without clinical improvement. Moreover, acetabular cup dislocation was documented. She underwent prosthesis explantation, debridement, and positioning of an antimicrobial mixed spacer. From the intraoperatory cultures S. epidermidis and Acinetobacter baumannii were grown. Daptomycin, ceftazidime, colistin and rifampin were administered. Four days later, rifampin was stopped due to a suspected liver toxicity. While undergoing therapy she presented recurrent episodes of wound dehiscence and on the 22nd week of treatment a further surgical debridement was performed, upon which the spacer was removed. At this time, intraoperative cultures resulted negative. Three months later, after a total of 8 months, antimicrobials were interrupted. Subsequently, a femoral transcondylar traction was positioned, and 3 weeks later a new prosthesis was reimplanted. At over 1 year after reimplantation she is well.
Our findings suggest that microbiologic investigations are mandatory even when prosthetic joint infection is not suspected. Molecular methods for identification of microorganisms can be used in addition to conventional cultures especially when patients are under antibiotic treatment. Daptomycin, ceftazidime and colistin can be administered for several months without side effects. Guidelines specifically addressing the diagnosis and the management of polymicrobial, multidrug-resistant prosthetic joint infections need to be developed.
人工关节感染是关节植入物的严重并发症。当涉及多种微生物和/或耐多药微生物时,会出现更多并发症。目前,关于这些感染的管理以及达托霉素、头孢他啶和黏菌素长期治疗的耐受性的数据有限。
一名55岁的白人女性因感染在1年前取出了右髋关节假体,此次因假体再植入入院。入院时,我院无法获取有关假体感染病因和治疗的既往病史。根据临床、实验室检查结果和影像学研究,未怀疑有感染。重新植入了髋关节假体。手术时,未进行组织病理学和微生物学检查。再植入三周后,诊断出因阴沟肠杆菌引起的手术部位感染,并开具了口服环丙沙星。四天后,发现假体周围有积液,经皮穿刺抽吸培养出表皮葡萄球菌和溶血葡萄球菌。同一样本中还检测到阴沟肠杆菌基因组。在环丙沙星基础上加用替考拉宁和美罗培南,但临床症状无改善。此外,记录到髋臼杯脱位。她接受了假体取出、清创,并放置了抗菌混合间隔物。术中培养出表皮葡萄球菌和鲍曼不动杆菌。给予达托霉素、头孢他啶、黏菌素和利福平治疗。四天后,因怀疑肝毒性停用利福平。在治疗过程中,她出现了伤口裂开的反复情况,在治疗的第22周进行了进一步的手术清创,取出了间隔物。此时,术中培养结果为阴性。三个月后,总共8个月后,停用抗菌药物。随后,进行了股骨髁上牵引,三周后重新植入了新的假体。再植入1年多后,她情况良好。
我们的研究结果表明,即使未怀疑人工关节感染,微生物学检查也是必要的。除传统培养外,还可使用分子方法鉴定微生物,尤其是在患者接受抗生素治疗时。达托霉素、头孢他啶和黏菌素可连续使用数月而无副作用。需要制定专门针对多种微生物、耐多药人工关节感染的诊断和管理指南。