Mullen Kerri-Anne, Coyle Douglas, Manuel Douglas, Nguyen Hai V, Pham Ba', Pipe Andrew L, Reid Robert D
Division of Prevention and Rehabilitation, University of Ottawa Heart Institute, Ottawa, Ontario, Canada.
Department of Epidemiology and Community Medicine, University of Ottawa, Ottawa, Ontario, Canada.
Tob Control. 2015 Sep;24(5):489-96. doi: 10.1136/tobaccocontrol-2013-051483. Epub 2014 Jun 16.
Cigarette smoking causes many chronic diseases that are costly and result in frequent hospitalisation. Hospital-initiated smoking cessation interventions increase the likelihood that patients will become smoke-free. We modelled the cost-effectiveness of the Ottawa Model for Smoking Cessation (OMSC), an intervention that includes in-hospital counselling, pharmacotherapy and posthospital follow-up, compared to usual care among smokers hospitalised with acute myocardial infarction (AMI), unstable angina (UA), heart failure (HF), and chronic obstructive pulmonary disease (COPD).
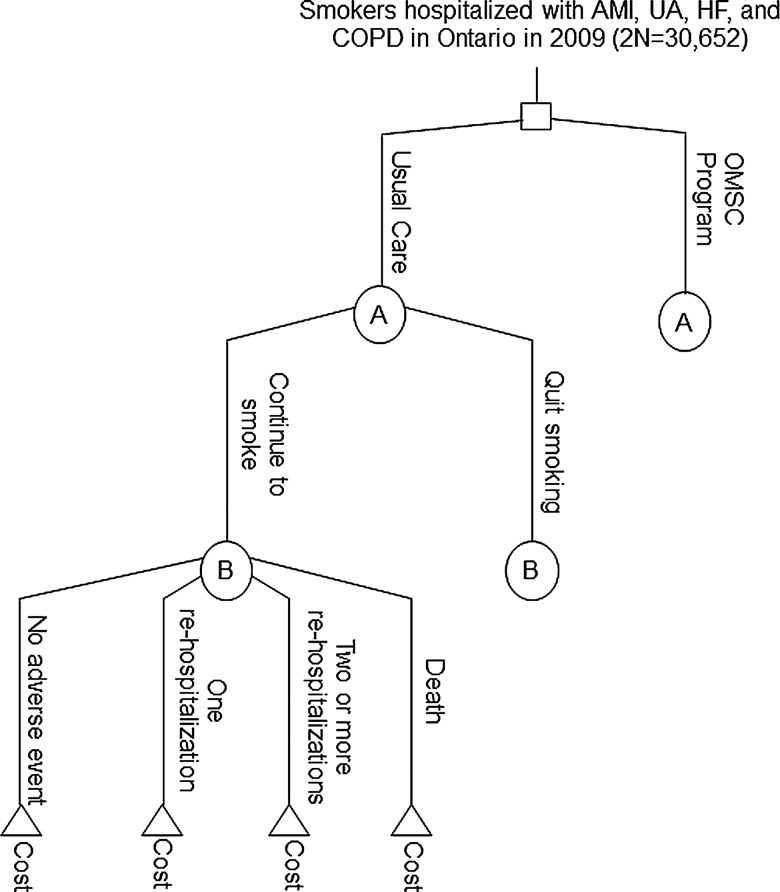
We completed a cost-effectiveness analysis based on a decision-analytic model to assess smokers hospitalised in Ontario, Canada for AMI, UA, HF, and COPD, their risk of continuing to smoke and the effects of quitting on re-hospitalisation and mortality over a 1-year period. We calculated short-term and long-term cost-effectiveness ratios. Our primary outcome was 1-year cost per quality-adjusted life year (QALY) gained.
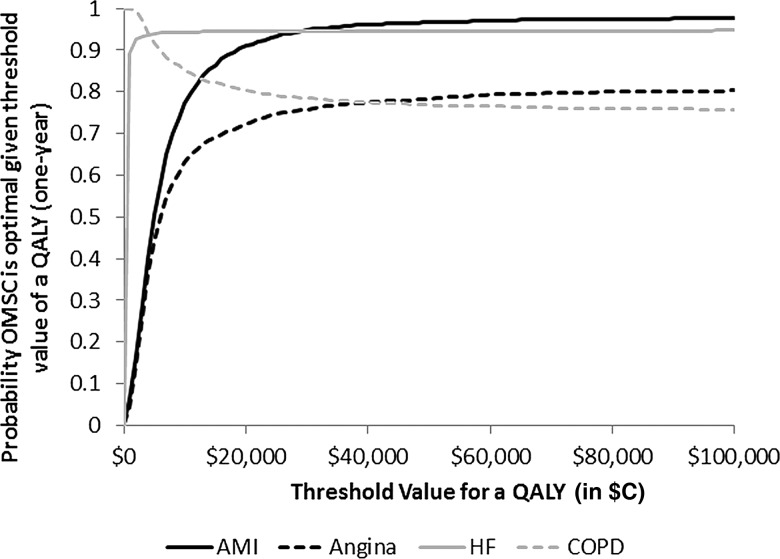
From the hospital payer's perspective, delivery of the OMSC can be considered cost effective with 1-year cost per QALY gained of $C1386, and lifetime cost per QALY gained of $C68. In the first year, we calculated that provision of the OMSC to 15 326 smokers would generate 4689 quitters, and would prevent 116 rehospitalisations, 923 hospital days, and 119 deaths. Results were robust within numerous sensitivity analyses.
The OMSC appears to be cost-effective from the hospital payer perspective. Important consideration is the relatively low intervention cost compared to the reduction in costs related to readmissions for illnesses associated with continued smoking.
吸烟会引发许多慢性疾病,这些疾病不仅成本高昂,还会导致频繁住院。医院发起的戒烟干预措施会增加患者戒烟的可能性。我们建立了渥太华戒烟模型(OMSC)的成本效益模型,该干预措施包括住院咨询、药物治疗和出院后随访,并将其与因急性心肌梗死(AMI)、不稳定型心绞痛(UA)、心力衰竭(HF)和慢性阻塞性肺疾病(COPD)住院的吸烟者的常规护理进行比较。
我们基于决策分析模型完成了一项成本效益分析,以评估在加拿大安大略省因AMI、UA、HF和COPD住院的吸烟者、他们继续吸烟的风险以及戒烟对1年内再次住院和死亡率的影响。我们计算了短期和长期成本效益比率。我们的主要结果是每获得一个质量调整生命年(QALY)的1年成本。
从医院支付方的角度来看,实施OMSC可被认为具有成本效益,每获得一个QALY的1年成本为1386加元,每获得一个QALY的终身成本为68加元。在第一年,我们计算得出,为15326名吸烟者提供OMSC将产生4689名戒烟者,并可预防116次再次住院、923个住院日和119例死亡。在众多敏感性分析中,结果都是稳健的。
从医院支付方的角度来看,OMSC似乎具有成本效益。重要的考虑因素是,与因持续吸烟相关疾病的再入院成本降低相比,干预成本相对较低。