Nesioonpour Sholeh, Akhondzadeh Reza, Mokmeli Soheila, Moosavi Shahnam, Mackie Mandana, Naderan Morteza
Pain Res Manag. 2014 Nov-Dec;19(6):e154-8. doi: 10.1155/2014/314910. Epub 2014 Jun 19.
The use of intravenous regional anesthesia (IVRA) is limited by pain resulting from the application of tourniquets and postoperative pain.
To assess the efficacy of low-level laser therapy added to IVRA for improving pain related to surgical fixation of distal radius fractures.
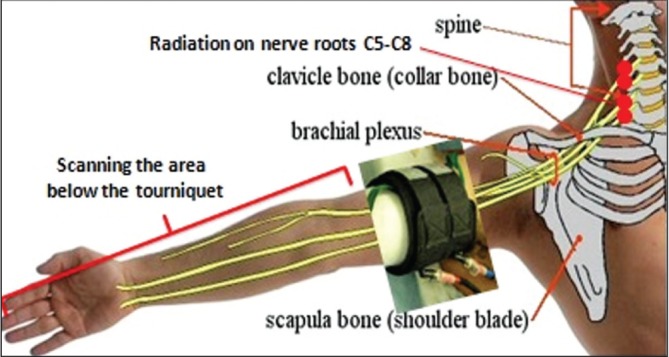
The present double-blinded, placebo-controlled, randomized clinical trial involved 48 patients who were undergoing surgical fixation of distal radius fractures. Participants were randomly assigned to either an intervention group (n=24), who received 808 nm laser irradiation as 4 J⁄point for 20 s over ipsilateral three nerve roots in the cervical region corresponding to C5-C8 vertebrae, and 808 nm laser irradiation as 0.1 J⁄cm2 for 5 min in a tangential scanning mode over the affected extremity; or a control group (n=24), who underwent the same protocol and timing of laser probe application with the laser switched off. Both groups received the same IVRA protocol using 2% lidocaine.
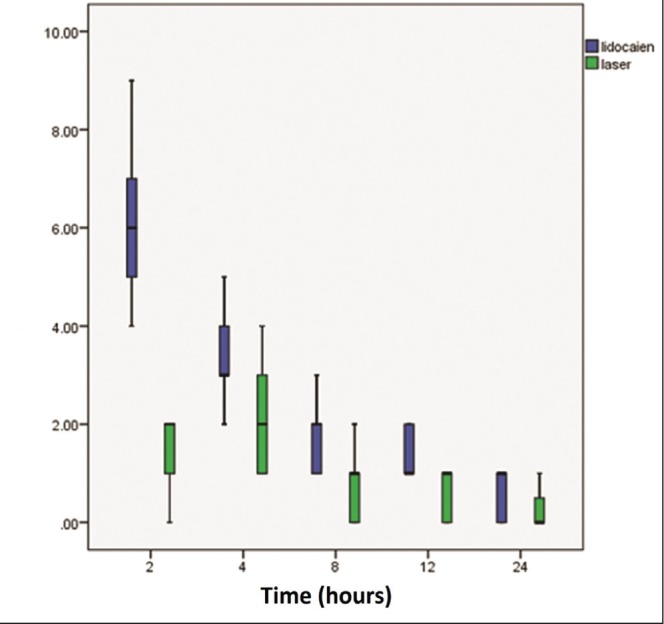
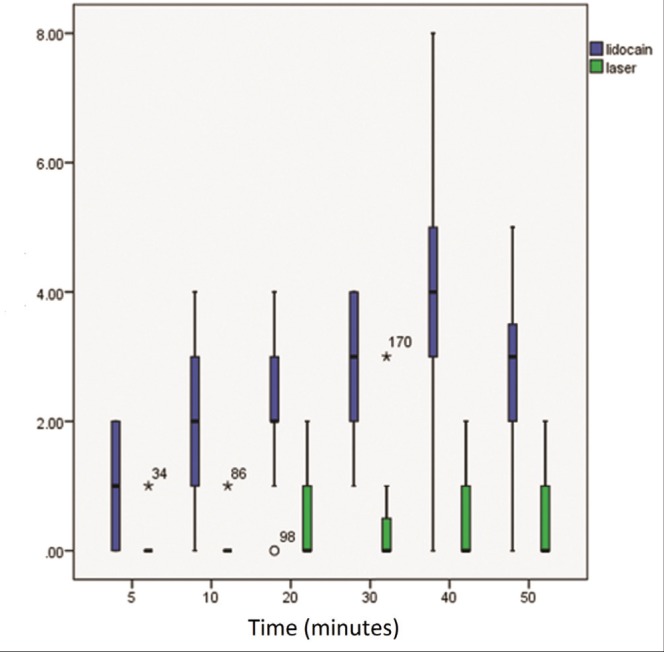
The mean visual analogue scale scores were significantly lower in the laser-assisted group than in the lidocaine-only group on all measurements during and after operation (P<0.05). The mean time to the first need for fentanyl administration during the operation was longer in the laser group (P=0.04). The total amount of fentanyl administered to patients was significantly lower in the laser-assisted group (P=0.003). The laser group needed significantly less pethidine for pain relief (P=0.001) and at a later time (P=0.002) compared with the lidocaine-only group. There was no difference between the groups in terms of mean arterial pressure and heart rate.
The addition of gallium-aluminum-arsenide laser irradiation to intravenous regional anesthesia is safe, and reduces pain during and after the operation.
静脉区域麻醉(IVRA)的应用受到止血带应用所致疼痛和术后疼痛的限制。
评估在IVRA基础上联合低强度激光治疗对改善桡骨远端骨折手术固定相关疼痛的疗效。
本双盲、安慰剂对照、随机临床试验纳入了48例接受桡骨远端骨折手术固定的患者。参与者被随机分为干预组(n = 24),该组在对应C5 - C8椎体的颈部同侧三根神经根处接受808 nm激光照射,剂量为4 J/点,持续20秒,并在患侧肢体以切线扫描模式接受808 nm激光照射,剂量为0.1 J/cm²,持续5分钟;或对照组(n = 24),该组接受相同的激光探头应用方案和时间,但激光关闭。两组均采用2%利多卡因进行相同的IVRA方案。
在手术期间和术后的所有测量中,激光辅助组的平均视觉模拟量表评分均显著低于单纯利多卡因组(P < 0.05)。手术期间首次需要使用芬太尼的平均时间在激光组更长(P = 0.04)。激光辅助组患者使用的芬太尼总量显著更低(P = 0.003)。与单纯利多卡因组相比,激光组缓解疼痛所需的哌替啶显著更少(P = 0.001),且用药时间更晚(P = 0.002)。两组在平均动脉压和心率方面无差异。
在静脉区域麻醉中添加砷化镓铝激光照射是安全的,并可减轻手术期间和术后的疼痛。