Modabber Ali, Ayoub Nassim, Möhlhenrich Stephan Christian, Goloborodko Evgeny, Sönmez Tolga Taha, Ghassemi Mehrangiz, Loberg Christina, Lethaus Bernd, Ghassemi Alireza, Hölzle Frank
Department of Oral, Maxillofacial and Plastic Facial Surgery, RWTH Aachen University Hospital, Aachen, Germany.
Department of Orthodontics, RWTH Aachen University Hospital, Aachen, Germany.
Med Devices (Auckl). 2014 Jun 16;7:211-7. doi: 10.2147/MDER.S62698. eCollection 2014.
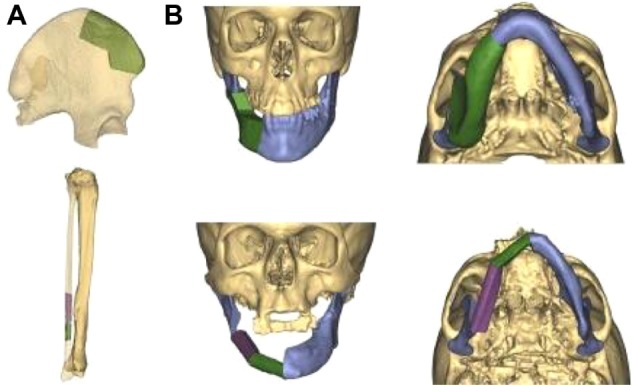
The intention of mandibular reconstruction is to restore the complex anatomy with maximum possible functionality and high accuracy. The aim of this study was to evaluate the accuracy of computer-assisted surgery in primary mandibular reconstruction with an iliac crest bone flap compared with an osteomyocutaneous fibula flap.
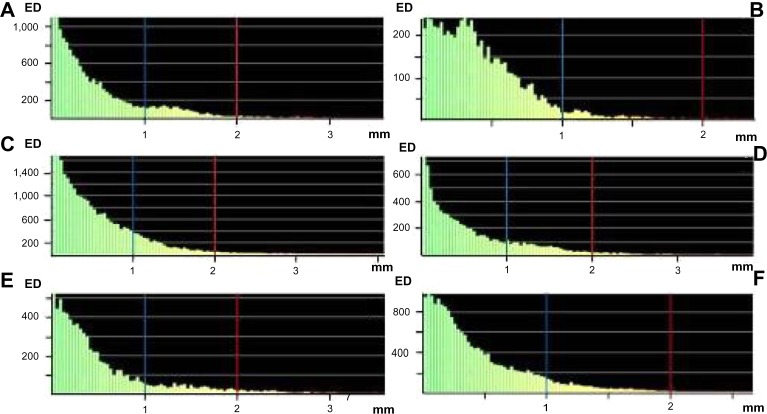
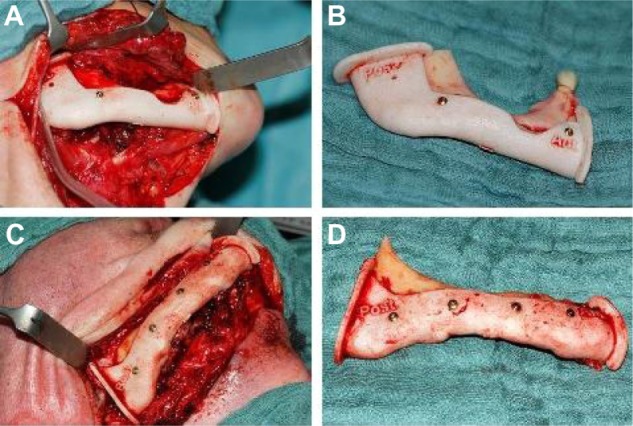
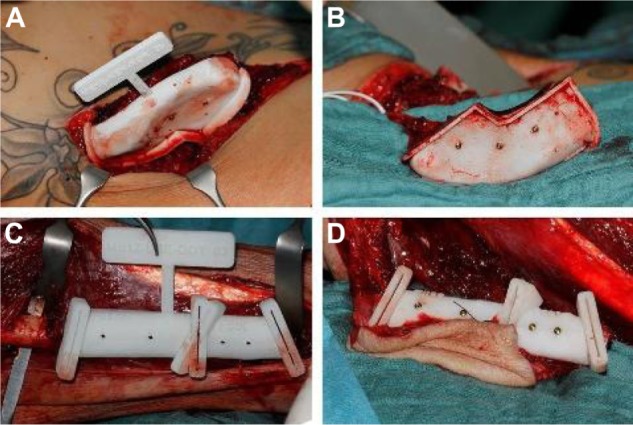
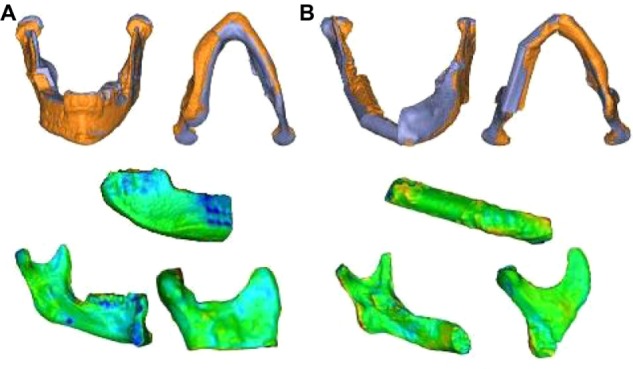
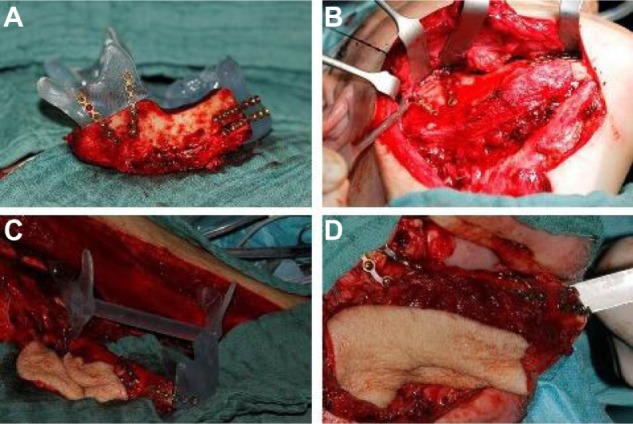
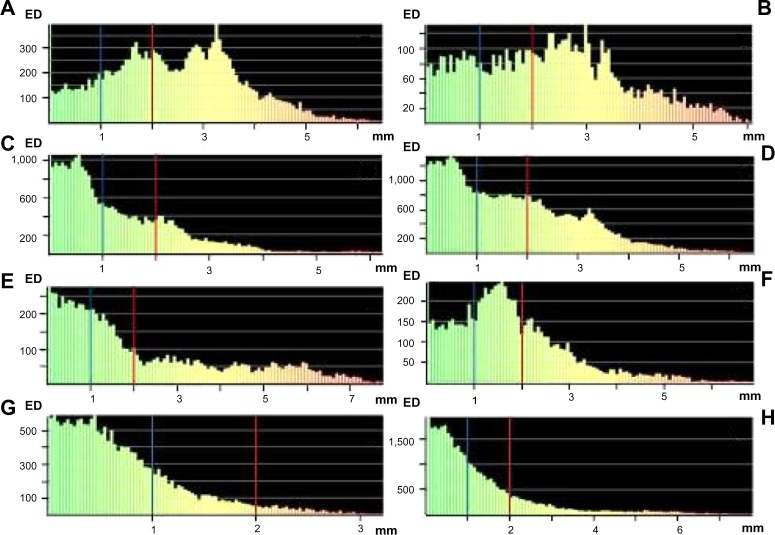
Preoperative computed tomography data of the mandible and the iliac crest or fibula donor site were imported into a specific surgical planning software program. Surgical guides were manufactured using a rapid prototyping technique for translating the virtual plan, including information on the transplant dimensions and shape, into real-time surgery. Using postoperative computed tomography scans and an automatic surface-comparison algorithm, the actual postoperative situation was compared with the preoperative virtual simulation.
The actual flap position showed a mean difference from the virtual plan of 2.43 mm (standard deviation [SD] ±1.26) and a surface deviation of 39% <2 mm and 15% <1 mm for the iliac crest bone flap, and a mean difference of 2.18 mm (SD ±1.93) and a surface deviation of 60% <2 mm and 37% <1 mm for the osteomyocutaneous fibula flap. The position of the neomandible reconstructed with an osteomyocutaneous fibula flap indicated a mean difference from the virtual plan of 1.25 mm (SD ±1.31) and a surface deviation of 82% <2 mm and 57% <1 mm, in contrast to a mean difference of 1.68 mm (SD ±1.25) and a surface deviation of 63% <2 mm and 38% <1 mm for the neomandible after reconstruction with an iliac crest bone flap. For shape analysis, a similarly high accuracy could be calculated for both flaps.
Virtual surgical planning is an effective method for mandibular reconstruction with vascularized bone flaps, and can help to restore the anatomy of the mandible with high accuracy in position and shape. It seems that primary mandibular reconstruction with the osteomyocutaneous fibula flap is more accurate compared with the vascularized iliac crest bone flap.
下颌骨重建的目的是尽可能以最大的功能和高精度恢复复杂的解剖结构。本研究的目的是评估与带血管蒂腓骨肌皮瓣相比,计算机辅助手术在髂嵴骨瓣一期下颌骨重建中的准确性。
将下颌骨及髂嵴或腓骨供区的术前计算机断层扫描数据导入特定的手术规划软件程序。使用快速成型技术制作手术导板,将虚拟计划(包括移植体尺寸和形状信息)转化为实时手术。利用术后计算机断层扫描和自动表面比较算法,将实际术后情况与术前虚拟模拟进行比较。
对于髂嵴骨瓣,实际皮瓣位置与虚拟计划的平均差异为2.43 mm(标准差[SD]±1.26),表面偏差<2 mm的占39%,<1 mm的占15%;对于带血管蒂腓骨肌皮瓣,平均差异为2.18 mm(SD±1.93),表面偏差<2 mm的占60%,<1 mm的占37%。带血管蒂腓骨肌皮瓣重建的新下颌骨位置与虚拟计划的平均差异为1.25 mm(SD±1.31),表面偏差<2 mm的占82%,<1 mm的占57%;相比之下,髂嵴骨瓣重建后新下颌骨的平均差异为1.68 mm(SD±1.25),表面偏差<2 mm的占63%,<1 mm的占38%。对于形状分析,两种皮瓣均可计算出相似的高精度。
虚拟手术规划是带血管化骨瓣进行下颌骨重建的有效方法,有助于高精度地恢复下颌骨的位置和形状。与带血管蒂髂嵴骨瓣相比,带血管蒂腓骨肌皮瓣一期下颌骨重建似乎更准确。