Fan Li, Sarnak Mark J, Tighiouart Hocine, Drew David A, Kantor Amy L, Lou Kristina V, Shaffi Kamran, Scott Tammy M, Weiner Daniel E
Division of Nephrology, Department of Medicine, Tufts Medical Center, Boston, Mass., USA.
Am J Nephrol. 2014;40(1):12-8. doi: 10.1159/000363539. Epub 2014 Jun 24.
There are limited data regarding the relationship between depression and mortality in hemodialysis (HD) patients.
Among 323 patients receiving maintenance HD, depression symptoms were assessed using the Center for Epidemiologic Studies Depression (CES-D) scale, with a score of ≥16 consistent with depression. Adjusted Cox proportional-hazards models with additional analyses incorporating antidepressant medication use were used to evaluate the association between depression and mortality. Baseline CES-D scores were used for the primary analyses, while secondary time-dependent analyses incorporated subsequent CES-D results.
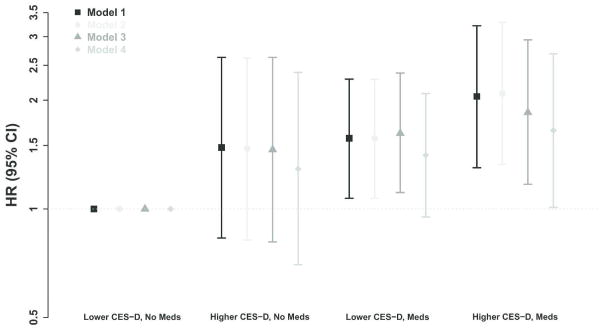
The mean age was 62.9 ± 16.5 years, 46% of the subjects were women and 22% were African-American. The mean baseline CES-D score was 10.7± 8.3, and 83 (26%) participants had CES-D scores ≥16. During a median (25th, 75th) follow-up of 25 (13, 43) months, 154 participants died. After adjusting for age, sex, race, primary cause of kidney failure, dialysis vintage and access, baseline depression was associated with an increased risk of all-cause mortality (HR 1.51 and 95% CI 1.06-2.17). This attenuated with further adjustment for cardiovascular disease, smoking, Kt/V, serum albumin, log C-reactive protein and use of antidepressants (HR 1.21 and 95% CI 0.82-1.80). When evaluating time-dependent CES-D, depression remained associated with increased mortality risk in the fully adjusted model (HR 1.44 and 95% CI 1.00-2.06).
Greater symptoms of depression are associated with an increased risk of mortality in HD patients, particularly when accounting for the most proximate assessment. This relationship was attenuated with adjustment for comorbid conditions, suggesting a complex relationship between clinical characteristics and depression symptoms. Future studies should evaluate whether treatment for depression impacts mortality among HD patients.
关于血液透析(HD)患者抑郁与死亡率之间的关系,相关数据有限。
在323例接受维持性血液透析的患者中,使用流行病学研究中心抑郁量表(CES-D)评估抑郁症状,得分≥16分则符合抑郁诊断。采用调整后的Cox比例风险模型,并结合抗抑郁药物使用情况进行额外分析,以评估抑郁与死亡率之间的关联。主要分析采用基线CES-D评分,而次要的时间依赖性分析纳入了后续的CES-D结果。
平均年龄为62.9±16.5岁,46%的受试者为女性,22%为非裔美国人。平均基线CES-D评分为10.7±8.3,83名(26%)参与者的CES-D评分≥16分。在中位(第25、75百分位数)随访25(13,43)个月期间,154名参与者死亡。在调整年龄、性别、种族、肾衰竭的主要病因、透析时间和血管通路后,基线抑郁与全因死亡率风险增加相关(风险比1.51,95%置信区间1.06-2.17)。在进一步调整心血管疾病、吸烟、Kt/V、血清白蛋白、对数C反应蛋白和抗抑郁药物使用情况后,这种关联减弱(风险比1.21,95%置信区间0.82-1.80)。在评估时间依赖性CES-D时,在完全调整模型中,抑郁仍与死亡率风险增加相关(风险比1.44,95%置信区间1.00-2.06)。
抑郁症状越严重,HD患者的死亡风险越高,尤其是在考虑最近一次评估时。在调整合并症后,这种关系减弱,表明临床特征与抑郁症状之间存在复杂关系。未来的研究应评估抑郁治疗是否会影响HD患者的死亡率。