Ursing Johan, Rombo Lars, Rodrigues Amabelia, Aaby Peter, Kofoed Poul-Erik
Projecto de Saúde de Bandim, Indepth Network, Bissau, Guinea-Bissau; Malaria Research Laboratory, Unit of Infectious Diseases, Department of Medicine, Karolinska University Hospital, Stockholm, Sweden; Department of microbiology, Tumor and Cell Biology, Karolinska Institutet, Solna, Sweden.
Malaria Research Laboratory, Unit of Infectious Diseases, Department of Medicine, Karolinska University Hospital, Stockholm, Sweden; Department of Infectious Diseases Mälarsjukhuset, Eskilstuna, Sweden; Centre for Clinical Research, Sörmland county council, Eskilstuna, Sweden.
PLoS One. 2014 Jul 1;9(7):e101167. doi: 10.1371/journal.pone.0101167. eCollection 2014.
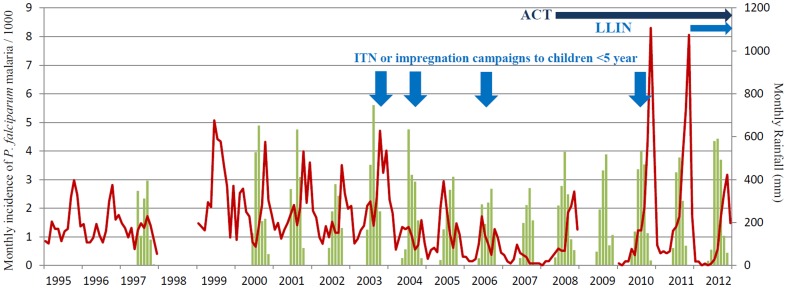
As Plasmodium falciparum prevalence decreases in many parts of Sub-Saharan Africa, so does immunity resulting in larger at risk populations and increased risk of malaria resurgence. In Bissau, malaria prevalence decreased from ∼50% to 3% between 1995 and 2003. The epidemiological characteristics of P. falciparum malaria within Bandim health and demographic surveillance site (population ∼100,000) between 1995 and 2012 are described.
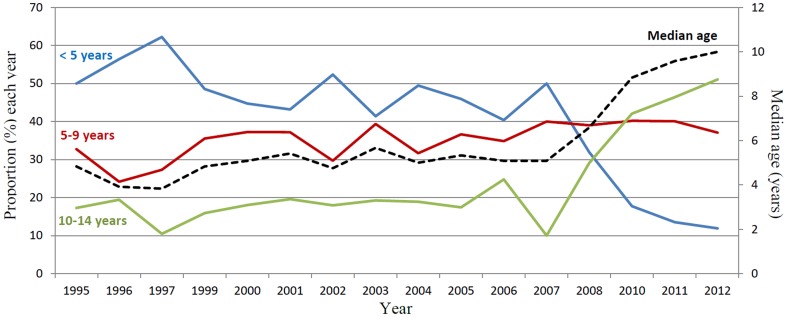
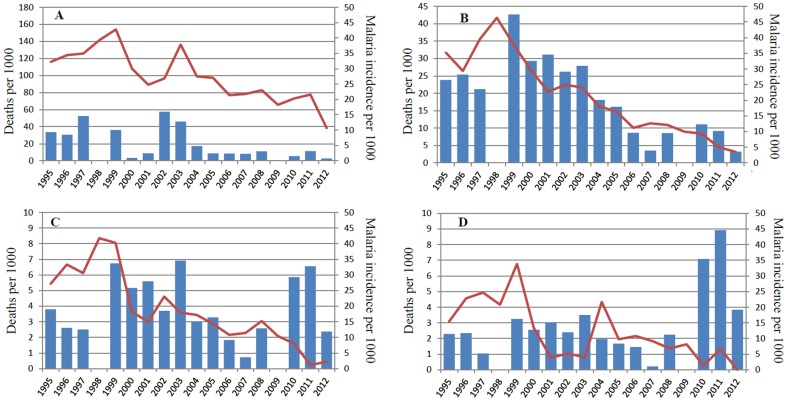
The population was determined by census. 3603 children aged <15 years that were enrolled in clinical trials at the Bandim health centre (1995-2012) were considered incident cases. The mean annual malaria incidence per thousand children in 1995-1997, 1999-2003, 2007, 2011, 2012 were as follows; age <5 years 22→29→4→9→3, age 5-9 years 15→28→4→33→12, age 10-14 years 9→15→1→45→19. There were 4 campaigns (2003-2010) to increase use of insecticide treated bed nets (ITN) amongst children <5 years. An efficacious high-dose chloroquine treatment regime was routinely used until artemisinin based combination therapy (ACT) was introduced in 2008. Long lasting insecticide treated bed nets (LLIN) were distributed in 2011. By 2012 there was 1 net per 2 people and 97% usage. All-cause mortality decreased from post-war peaks in 1999 until 2012 in all age groups and was not negatively affected by malaria resurgence.
The cause of decreasing malaria incidence (1995-2007) was probably multifactorial and coincident with the use of an efficacious high-dose chloroquine treatment regime. Decreasing malaria prevalence created a susceptible group of older children in which malaria resurged, highlighting the need to include all age groups in malaria interventions. ACT did not hinder malaria resurgence. Mass distribution of LLINs probably curtailed malaria epidemics. All-cause mortality was not negatively affected by malaria resurgence.
随着撒哈拉以南非洲许多地区恶性疟原虫流行率的下降,免疫力也随之下降,导致高危人群增多,疟疾复发风险增加。在比绍,1995年至2003年间,疟疾流行率从约50%降至3%。本文描述了1995年至2012年间班迪姆健康与人口监测点(人口约10万)内恶性疟原虫疟疾的流行病学特征。
通过人口普查确定人口数量。将在班迪姆健康中心参加临床试验(1995 - 2012年)的3603名15岁以下儿童视为新发病例。1995 - 1997年、1999 - 2003年、2007年、2011年、2012年每千名儿童的年疟疾发病率如下:5岁以下儿童为22→29→4→9→3,5 - 9岁儿童为15→28→4→33→12,10 - 14岁儿童为9→15→1→45→19。开展了4次活动(2003 - 2010年)以增加5岁以下儿童对经杀虫剂处理蚊帐(ITN)的使用。在2008年引入以青蒿素为基础的联合疗法(ACT)之前,常规使用有效的高剂量氯喹治疗方案。2011年分发了长效经杀虫剂处理蚊帐(LLIN)。到2012年,每两人有1顶蚊帐,使用率为97%。所有年龄组的全因死亡率从1999年的战后峰值降至2012年,且未受到疟疾复发的负面影响。
疟疾发病率下降(1995 - 2007年)的原因可能是多因素的,且与使用有效的高剂量氯喹治疗方案同时发生。疟疾流行率下降导致大龄儿童成为易感人群,疟疾在其中复发,这凸显了在疟疾干预措施中纳入所有年龄组的必要性。ACT并未阻碍疟疾复发。大规模分发LLINs可能遏制了疟疾流行。全因死亡率未受到疟疾复发的负面影响。