The Royal Marsden Hospital, Fulham Road, London SW3 6JJ, UK.
Institut Català d'Oncologia L'Hospitalet, Genitourinary Tumors, Sarcoma and Melanoma Unit, Avda Gran Via 199, L'Hospitalet, 08908 Barcelona, Spain.
Br J Cancer. 2014 Aug 26;111(5):858-65. doi: 10.1038/bjc.2014.370. Epub 2014 Jul 8.
We conducted a phase I study in patients with advanced solid tumours to identify the recommended dose, assess pharmacokinetics (PK), pharmacodynamic activity and preclinical antitumour efficacy of the combination of sirolimus and gemcitabine.
Nineteen patients were treated with sirolimus 2 or 5 mg daily and gemcitabine 800 or 1000 mg m(-2) on days 1 and 8. Dose escalation depended on dose-limiting toxicity (DLT) rate during the first 3-week period. Paired skin biopsies were evaluated for phosphorylated S6 (pS6) as marker of mTOR (mammalian target of rapamycin) inhibition. Pharmacokinetics and preclinical evaluation of efficacy using two different sarcoma cell lines and leiomyosarcoma xenografts were also conducted.
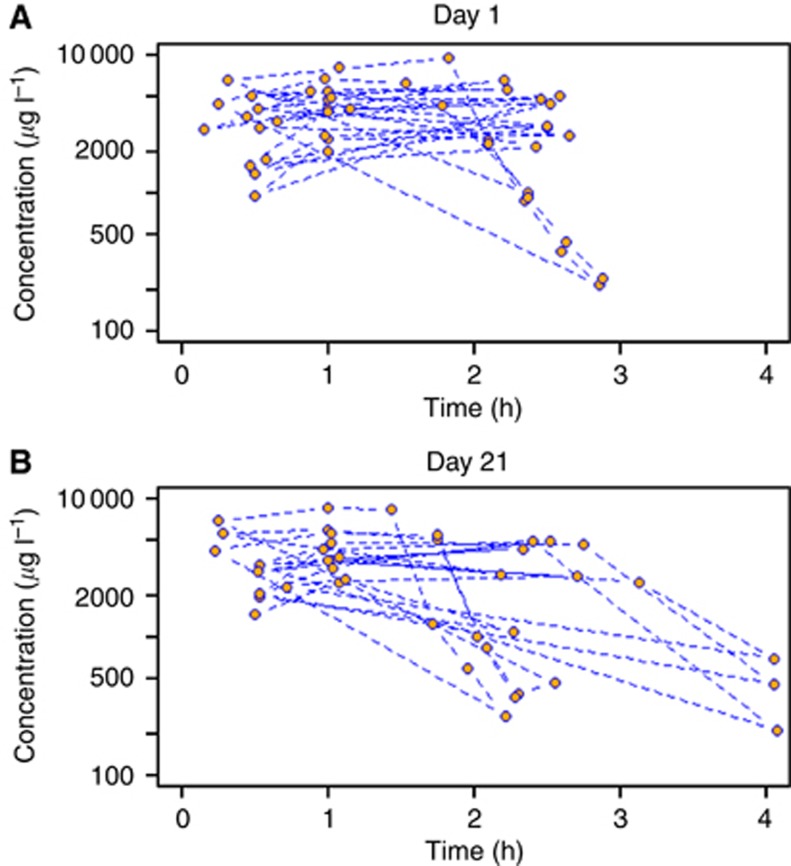
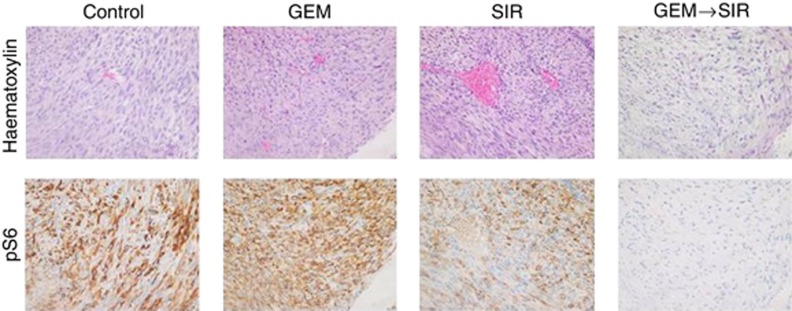
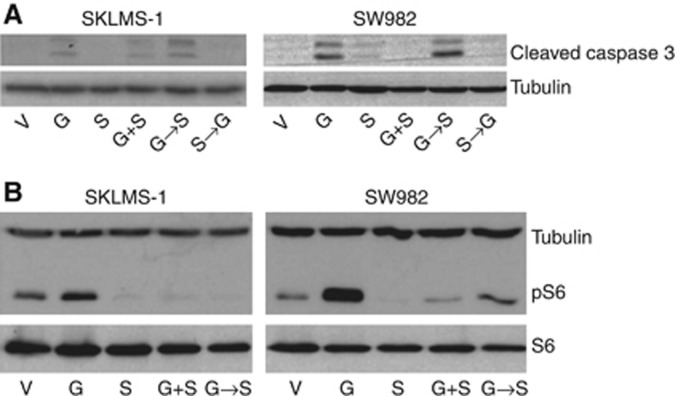
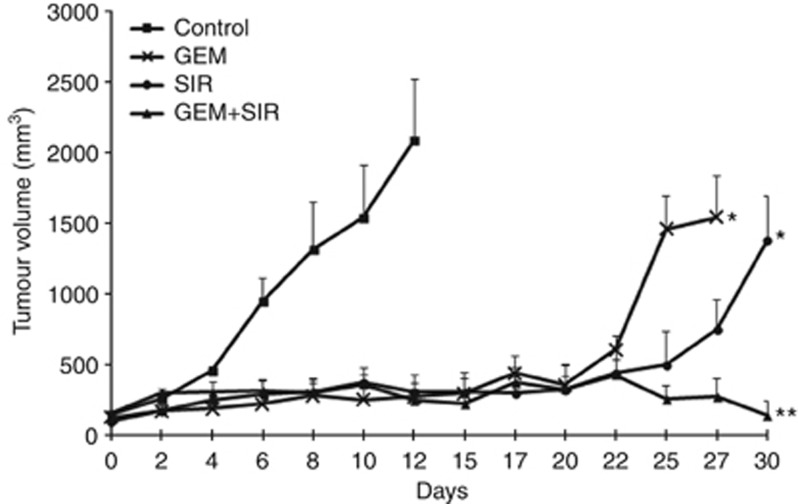
Three DLTs were observed: grade 3 transaminitis, grade 3 thrombocytopenia and grade 4 thrombocytopenia. Common treatment-related adverse events included anaemia, neutropenia, thrombocytopenia and transaminitis. Pharmacodynamic analyses demonstrated mTOR inhibition with sirolimus 5 mg and PK showed no influence of sirolimus concentrations on gemcitabine clearance. In vitro and in vivo studies suggested mTOR pathway hyperactivation by gemcitabine that was reversed by sirolimus. Tumour growth in leiomyosarcoma xenografts was dramatically inhibited by the treatment.
Recommended dose was sirolimus 5 mg per 24 h plus gemcitabine 800 mg m(-2). Antitumour activity in preclinical sarcoma models and mTOR signalling inhibition were observed. A phase II study is currently ongoing.
我们在晚期实体瘤患者中进行了一项 I 期研究,以确定西罗莫司联合吉西他滨的推荐剂量、评估药代动力学(PK)、药效学活性和临床前抗肿瘤疗效。
19 名患者接受西罗莫司 2 或 5mg/d 和吉西他滨 800 或 1000mg/m2 治疗,于第 1 天和第 8 天给药。剂量递增取决于前 3 周期间的剂量限制性毒性(DLT)发生率。用配对皮肤活检评估磷酸化 S6(pS6)作为 mTOR(哺乳动物雷帕霉素靶蛋白)抑制的标志物。还进行了使用两种不同的肉瘤细胞系和 leiomyosarcoma 异种移植进行的药效学 PK 评估和临床前疗效评估。
观察到 3 例 DLT:3 级转氨酶升高、3 级血小板减少和 4 级血小板减少。常见的治疗相关不良事件包括贫血、中性粒细胞减少、血小板减少和转氨酶升高。药效学分析表明西罗莫司 5mg 可抑制 mTOR,PK 显示西罗莫司浓度对吉西他滨清除率无影响。体外和体内研究表明,吉西他滨可导致 mTOR 通路过度激活,而西罗莫司可逆转这一作用。leiomyosarcoma 异种移植瘤的肿瘤生长受到显著抑制。
推荐的剂量为西罗莫司 24 小时 5mg 加吉西他滨 800mg/m2。在临床前肉瘤模型中观察到抗肿瘤活性和 mTOR 信号通路抑制。目前正在进行一项 II 期研究。