Xie Gaoqiang, Laskowitz Daniel T, Turner Elizabeth L, Egger Joseph R, Shi Ping, Ren Fuxiu, Gao Wei, Wu Yangfeng
Peking University Clinical Research Institute, Beijing, People's Republic of China.
Department of Neurology, Duke University Medicine Center, Durham, North Carolina, United States of America.
PLoS One. 2014 Jul 9;9(7):e101527. doi: 10.1371/journal.pone.0101527. eCollection 2014.
Health-related quality of life (HRQOL) may be associated with the longevity of patients; yet it is not clear whether this association holds in a general population, especially in low- and middle-income countries. The objective of this study was to determine whether baseline HRQOL was associated with 10-year all-cause mortality in a Chinese general population.
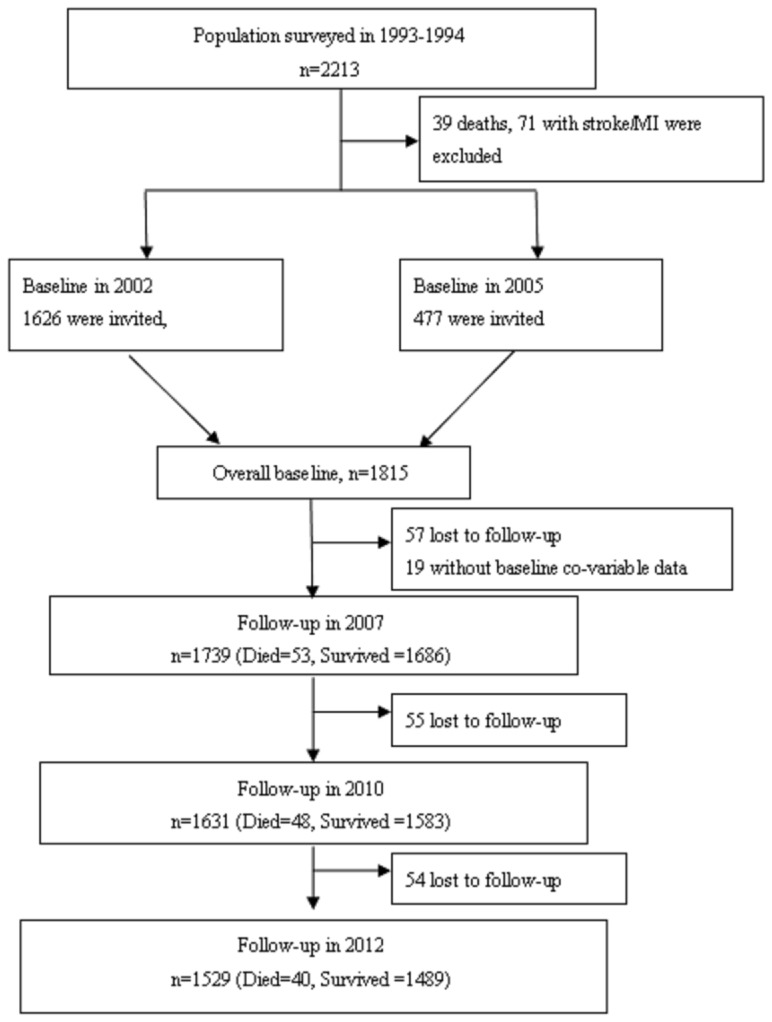
A prospective cohort study was conducted from 2002 to 2012 on 1739 participants in 11 villages of Beijing. Baseline data on six domains of HRQOL, chronic diseases and cardiovascular risk factors were collected in either 2002 (n = 1290) or 2005 (n = 449). Subjects were followed through the end of the study period, or until they were censored due to death or loss to follow-up, whichever came first.
A multivariable Cox model estimated that Total HRQOL score (bottom 50% versus top 50%) was associated with a 44% increase in all-cause mortality (Hazard Ratio [HR] = 1.44; 95% confidence interval [CI]: 1.00-2.06), after adjusting for sex, age, education levels, occupation, marital status, smoking status, fruit intake, vegetable intake, physical exercise, hypertension, history of a stroke, myocardial infarction, chronic respiratory disease, and kidney disease. Among the six HRQOL domains, the Independence domain had the largest fully adjusted HR (HR = 1.66; 95% CI: 1.13-2.42), followed by Psychological (HR = 1.47; 95% CI: 1.03-2.09), Environmental (HR = 1.43, 95% CI: 1.003-2.03), Physical (HR = 1.38; 95% CI: 0.97-1.95), General (HR = 1.37; 95% CI: 0.97-1.94), and the Social domain (HR = 1.15; 95% CI: 0.81-1.65).
Lower HRQOL, especially the inability to live independently, was associated with a significantly increased risk of 10-year all-cause mortality. The inclusion of HRQOL measures in clinical assessment may improve diagnostic accuracy to improve clinical outcomes and better target public health promotions.
健康相关生活质量(HRQOL)可能与患者的寿命相关;然而,这种关联在普通人群中是否成立尚不清楚,尤其是在低收入和中等收入国家。本研究的目的是确定中国普通人群的基线HRQOL是否与10年全因死亡率相关。
2002年至2012年对北京11个村庄的1739名参与者进行了一项前瞻性队列研究。在2002年(n = 1290)或2005年(n = 449)收集了关于HRQOL六个领域、慢性病和心血管危险因素的基线数据。对受试者进行随访,直至研究期结束,或因死亡或失访而被 censored,以先发生者为准。
多变量Cox模型估计,在调整了性别、年龄、教育水平、职业、婚姻状况、吸烟状况、水果摄入量、蔬菜摄入量、体育锻炼、高血压、中风史、心肌梗死、慢性呼吸道疾病和肾脏疾病后,总HRQOL得分(最低50%与最高50%)与全因死亡率增加44%相关(风险比[HR]=1.44;95%置信区间[CI]:1.00 - 2.06)。在六个HRQOL领域中,独立领域的完全调整后HR最大(HR = 1.66;95% CI:1.13 - 2.42),其次是心理领域(HR = 1.47;95% CI:1.03 - 2.09)、环境领域(HR = 1.43,95% CI:1.003 - 2.03)、身体领域(HR = 1.38;95% CI:0.97 - 1.95)、总体领域(HR = 1.37;95% CI:0.97 - 1.94)和社会领域(HR = 1.15;95% CI:0.81 - 1.65)。
较低的HRQOL,尤其是无法独立生活,与10年全因死亡率风险显著增加相关。将HRQOL测量纳入临床评估可能会提高诊断准确性,以改善临床结果并更好地针对公共卫生促进。