Mello Bruno Henrique Gallindo de, Oliveira Gustavo Bernardes F, Ramos Rui Fernando, Lopes Bernardo Baptista C, Barros Cecília Bitarães S, Carvalho Erick de Oliveira, Teixeira Fabio Bellini P, Arruda Guilherme D'Andréa S, Revelo Maria Sol Calero, Piegas Leopoldo Soares
Instituto Dante Pazzanese de Cardiologia, São Paulo, SP, Brazil.
Arq Bras Cardiol. 2014 Aug;103(2):107-17. doi: 10.5935/abc.20140091. Epub 2014 Jul 9.
The classification or index of heart failure severity in patients with acute myocardial infarction (AMI) was proposed by Killip and Kimball aiming at assessing the risk of in-hospital death and the potential benefit of specific management of care provided in Coronary Care Units (CCU) during the decade of 60.
To validate the risk stratification of Killip classification in the long-term mortality and compare the prognostic value in patients with non-ST-segment elevation MI (NSTEMI) relative to patients with ST-segment elevation MI (STEMI), in the era of reperfusion and modern antithrombotic therapies.
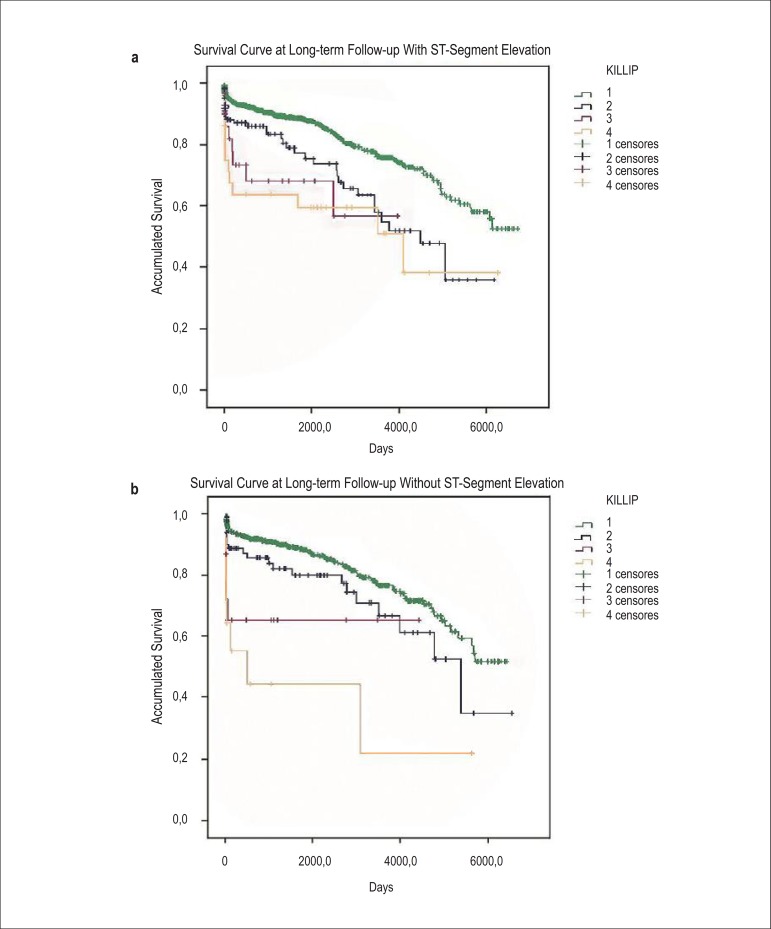
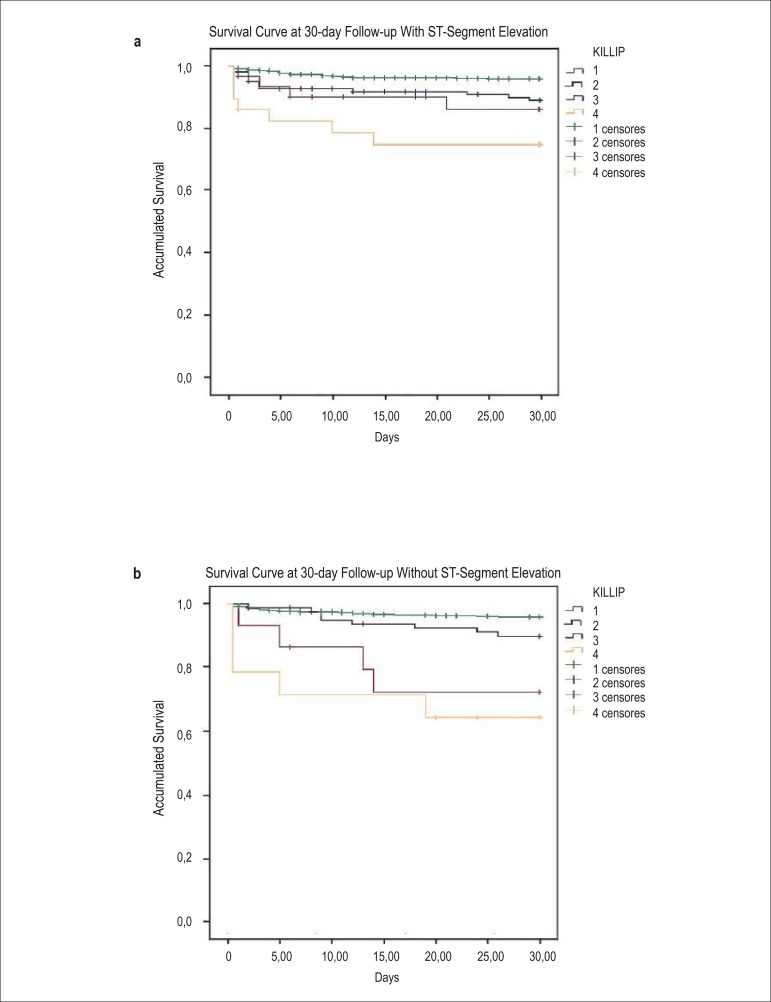
We evaluated 1906 patients with documented AMI and admitted to the CCU, from 1995 to 2011, with a mean follow-up of 05 years to assess total mortality. Kaplan-Meier (KM) curves were developed for comparison between survival distributions according to Killip class and NSTEMI versus STEMI. Cox proportional regression models were developed to determine the independent association between Killip class and mortality, with sensitivity analyses based on type of AMI.
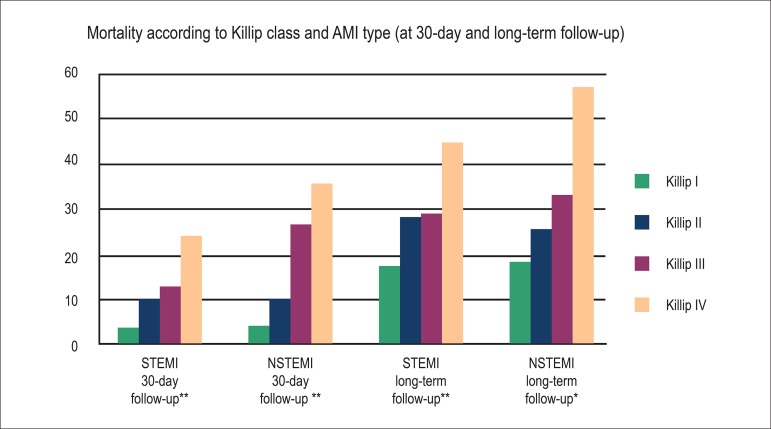
The proportions of deaths and the KM survival distributions were significantly different across Killip class >1 (p <0.001) and with a similar pattern between patients with NSTEMI and STEMI. Cox models identified the Killip classification as a significant, sustained, consistent predictor and independent of relevant covariables (Wald χ2 16.5 [p = 0.001], NSTEMI) and (Wald χ2 11.9 [p = 0.008], STEMI).
The Killip and Kimball classification performs relevant prognostic role in mortality at mean follow-up of 05 years post-AMI, with a similar pattern between NSTEMI and STEMI patients.
急性心肌梗死(AMI)患者心力衰竭严重程度的分类或指数由基利普(Killip)和金博尔(Kimball)提出,旨在评估20世纪60年代冠心病监护病房(CCU)住院死亡风险以及特定护理管理的潜在益处。
在再灌注和现代抗栓治疗时代,验证基利普分类在长期死亡率方面的风险分层,并比较非ST段抬高型心肌梗死(NSTEMI)患者与ST段抬高型心肌梗死(STEMI)患者的预后价值。
我们评估了1995年至2011年入住CCU的1906例有记录的AMI患者,平均随访5年以评估总死亡率。绘制了Kaplan-Meier(KM)曲线,以比较根据基利普分级以及NSTEMI与STEMI的生存分布情况。建立Cox比例回归模型以确定基利普分级与死亡率之间的独立关联,并基于AMI类型进行敏感性分析。
基利普分级>1时,死亡比例和KM生存分布存在显著差异(p<0.001),NSTEMI患者和STEMI患者之间具有相似模式。Cox模型确定基利普分类是一个显著、持续、一致的预测指标,且独立于相关协变量(Wald χ2 16.5 [p = 0.001],NSTEMI)和(Wald χ2 11.9 [p = 0.008],STEMI)。
基利普和金博尔分类在AMI后平均5年随访的死亡率方面具有相关的预后作用,NSTEMI患者和STEMI患者之间具有相似模式。