Mathews William C, Agmas Wollelaw, Cachay Edward R, Cosman Bard C, Jackson Christopher
Department of Medicine, University of California San Diego, San Diego, California, United States of America.
Department of Surgery, University of California San Diego, San Diego, California, United States of America.
PLoS One. 2014 Aug 7;9(8):e104116. doi: 10.1371/journal.pone.0104116. eCollection 2014.
(1) To model the natural history of anal neoplasia in HIV-infected patients using a 3-state Markov model of anal cancer pathogenesis, adjusting for cytology misclassification; and (2) to estimate the effects of selected time-varying covariates on transition probabilities.
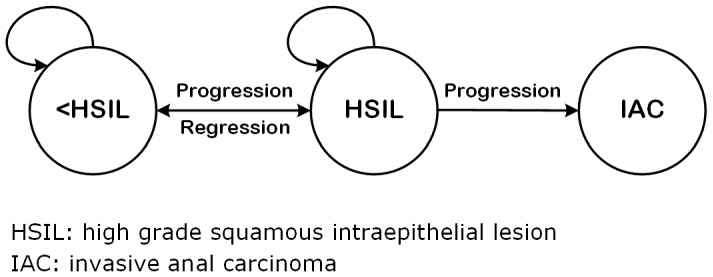
A retrospective cytology-based inception screening cohort of HIV-infected adults was analyzed using a 3-state Markov model of clinical pathogenesis of anal neoplasia.
Longitudinally ascertained cytology categories were adjusted for misclassification using estimates of cytology accuracy derived from the study cohort. Time-varying covariate effects were estimated as hazard ratios.
(1) There was a moderate to high probability of regression of the high grade squamous intraepithelial lesion (HSIL) state (27-62%) at 2 years after initial cytology screening; (2) the probability of developing invasive anal cancer (IAC) during the first 2 years after a baseline HSIL cytology is low (1.9-2.8%); (3) infrared coagulation (IRC) ablation of HSIL lesions is associated with a 2.2-4.2 fold increased probability of regression to <HSIL; and (4) antiretroviral therapy, suppressed HIV plasma viral load, and CD4 ≥350/mm3 are each associated with reduced probability of progression from <HSIL to HSIL.
The finding of moderate to high rates of regression of the HSIL state accompanied by low rates of progression to IAC should inform both screening and precursor treatment guideline development. There appears to be a consistent and robust beneficial effect of antiretroviral therapy, suppressed viral load, and higher CD4 on the transition from the <HSIL state to the HSIL state.
(1)使用肛门癌发病机制的三状态马尔可夫模型对HIV感染患者肛门肿瘤的自然史进行建模,并对细胞学错误分类进行校正;(2)估计选定的随时间变化的协变量对转移概率的影响。
采用肛门肿瘤临床发病机制的三状态马尔可夫模型,对一个基于细胞学的HIV感染成人回顾性起始筛查队列进行分析。
利用从研究队列中得出的细胞学准确性估计值,对纵向确定的细胞学类别进行错误分类校正。将随时间变化的协变量效应估计为风险比。
(1)在初次细胞学筛查后2年,高级别鳞状上皮内病变(HSIL)状态有中度到高度的消退概率(27%-62%);(2)在基线HSIL细胞学检查后的头2年内发生浸润性肛门癌(IAC)的概率较低(1.9%-2.8%);(3)HSIL病变的红外凝固(IRC)消融与回归至<HSIL的概率增加2.2至4.2倍相关;(4)抗逆转录病毒治疗、HIV血浆病毒载量被抑制以及CD4≥350/mm³均与从<HSIL进展至HSIL的概率降低相关。
HSIL状态有中度到高度的消退率且进展至IAC的比率较低这一发现,应为筛查和前驱病变治疗指南的制定提供依据。抗逆转录病毒治疗、病毒载量被抑制以及较高的CD4水平似乎对从<HSIL状态向HSIL状态的转变具有一致且强大的有益作用。