Zhang Xu-Feng, Yin Guo-Zhi, Liu Qing-Guang, Liu Xue-Min, Wang Bo, Yu Liang, Liu Si-Nan, Cui Hong-Ying, Lv Yi
Department of Hepatobiliary Surgery (X-FZ, G-ZY, Q-GL, X-ML, BW, LY, S-NL, YL); Institute of Advanced Surgical Technology and Engineering (X-FZ, X-ML, YL); Department of Chinese Acupuncture and Moxibustion, First Affiliated Hospital of Medical College, Xi'an Jiaotong University (H-YC), Xi'an, China.
Medicine (Baltimore). 2014 Aug;93(7):e48. doi: 10.1097/MD.0000000000000048.
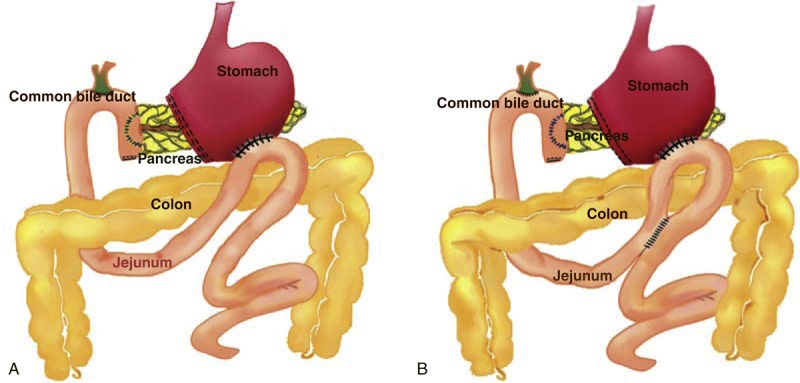
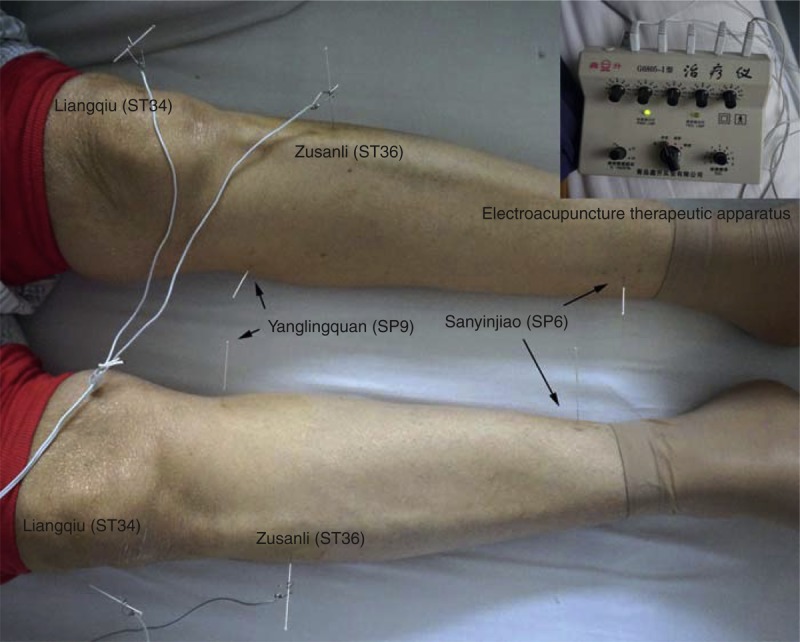
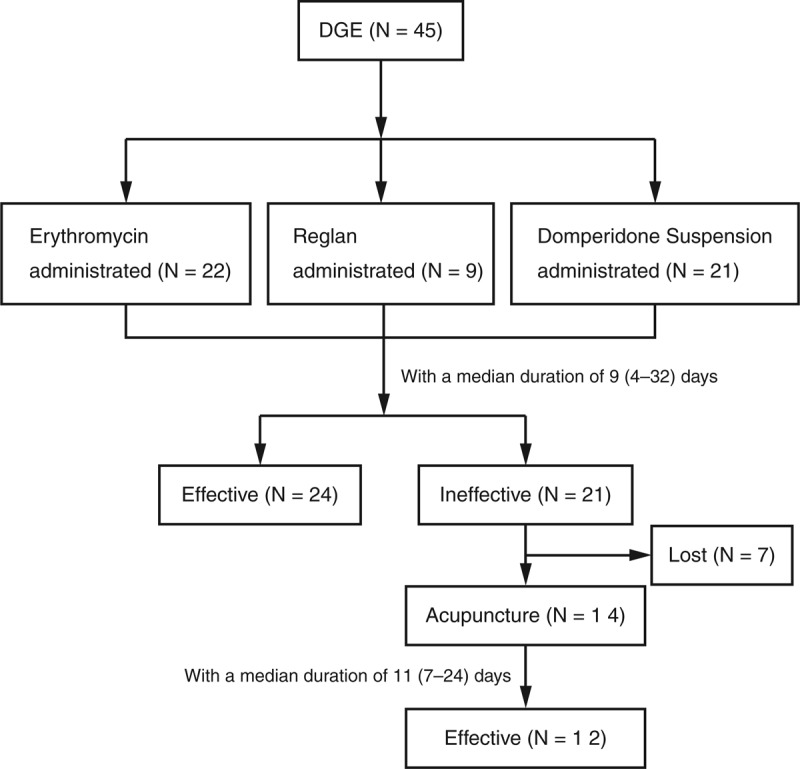
Whether an additional Braun enteroenterostomy is necessary in reducing delayed gastric emptying (DGE) after pancreaticoduodenectomy (PD) has not yet been well investigated. Herein, in this retrospective study, 395 consecutive cases of patients undergoing classic PD from 2009 to 2013 were reviewed. Patients with and without Braun enteroenterostomy were compared in preoperative baseline characteristics, surgical procedure, postoperative diagnosis, and morbidity including DGE. The DGE was defined and classified by the International Study Group of Pancreatic Surgery recommendation. The incidence of DGE was similar in patients with or without Braun enteroenterostomy following PD (37/347, 10.7% vs 8/48, 16.7%, P = 0.220). The patients in the 2 groups were not different in patient characteristics, lesions, surgical procedure, or postoperative complications, although patients without Braun enteroenterostomy more frequently presented postoperative vomiting than those with Braun enteroenterostomy (33.3% vs 15.3%, P = 0.002). Bile leakage, pancreatic fistula, and intraperitoneal abscess were risk factors for postoperative DGE (all P < 0.05). Prokinetic agents and acupuncture were effective in symptom relief of DGE in 24 out of 45 patients and 12 out of 14 patients, respectively.The additional Braun enteroenterostomy following classic PD was not associated with a decreased rate of DGE. Postoperative abdominal complications were strongly correlated with the onset of DGE. Prokinetic agents and acupuncture could be utilized in some patients with DGE.
在胰十二指肠切除术(PD)后,额外进行 Braun 肠肠吻合术对于减少胃排空延迟(DGE)是否必要尚未得到充分研究。在此回顾性研究中,我们回顾了 2009 年至 2013 年连续 395 例行经典 PD 的患者病例。比较了有和没有进行 Braun 肠肠吻合术患者的术前基线特征、手术过程、术后诊断以及包括 DGE 在内的发病率。DGE 根据国际胰腺手术研究组的建议进行定义和分类。PD 后有或没有进行 Braun 肠肠吻合术的患者中 DGE 的发生率相似(347 例中有 37 例,10.7% 对 48 例中有 8 例,16.7%,P = 0.220)。两组患者在患者特征、病变、手术过程或术后并发症方面无差异,尽管没有进行 Braun 肠肠吻合术的患者术后呕吐比进行了该手术的患者更频繁(33.3% 对 15.3%,P = 0.002)。胆漏、胰瘘和腹腔脓肿是术后 DGE 的危险因素(所有 P < 0.05)。促动力药物和针灸分别对 45 例患者中的 24 例和 14 例患者中的 12 例 DGE 症状缓解有效。经典 PD 后额外进行 Braun 肠肠吻合术与 DGE 发生率降低无关。术后腹部并发症与 DGE 的发生密切相关。促动力药物和针灸可用于一些 DGE 患者。