Torres Orlando Jorge M, Fernandes Eduardo de Souza M, Vasques Rodrigo Rodrigues, Waechter Fabio Luís, Amaral Paulo Cezar G, Rezende Marcelo Bruno de, Costa Roland Montenegro, Montagnini André Luís
Department of Surgery, Federal University of Maranhão, São Luis, MA.
Federal University of Rio de Janeiro, Rio de Janeiro, RJ.
Arq Bras Cir Dig. 2017 Jul-Sep;30(3):190-196. doi: 10.1590/0102-6720201700030007.
Pancreatoduodenectomy is a technically challenging surgical procedure with an incidence of postoperative complications ranging from 30% to 61%. The procedure requires a high level of experience, and to minimize surgery-related complications and mortality, a high-quality standard surgery is imperative.
To understand the Brazilian practice patterns for pancreatoduodenectomy.
A questionnaire was designed to obtain an overview of the surgical practice in pancreatic cancer, specific training, and experience in pancreatoduodenectomy. The survey was sent to members who declared an interest in pancreatic surgery.
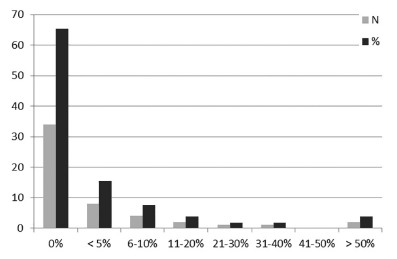
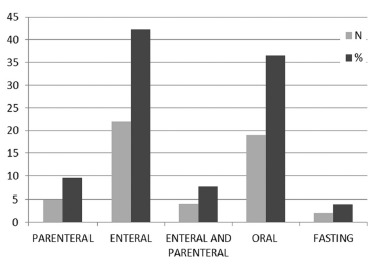
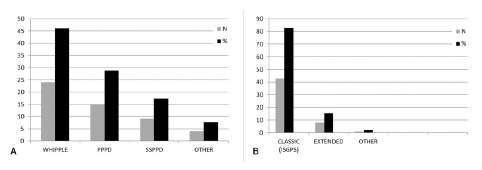
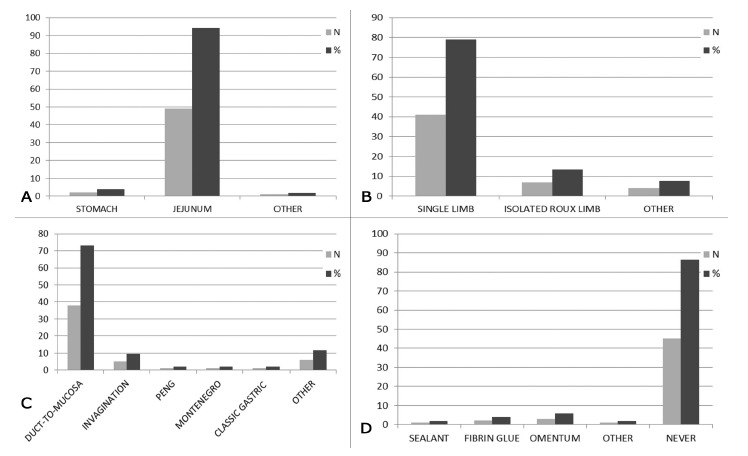
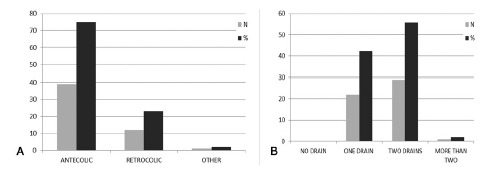
A total of 60 questionnaires were sent, and 52 have returned (86.7%). The Southeast had the most survey respondents, with 25 surgeons (48.0%). Only two surgeons (3.9%) performed more than 50% of their pancreatoduodenectomies by laparoscopy. A classic Whipple procedure was performed by 24 surgeons (46.2%) and a standard International Study Group on Pancreatic Surgery lymphadenectomy by 43 surgeons (82.7%). For reconstruction, pancreaticojejunostomy was performed by 49 surgeons (94.2%), single limb technique by 41(78.9%), duct-to-mucosa anastomosis by 38 (73.1%), internal trans-anastomotic stenting by 26 (50.0%), antecolic route of gastric reconstruction by 39 (75.0%), and Braun enteroenterostomy was performed by only six surgeons (11.5%). Prophylactic abdominal drainage was performed by all surgeons, and somatostatin analogues were utilized by six surgeons (11.5%). Early postoperative enteral nutrition was routine for 22 surgeons (42.3%), and 34 surgeons (65.4%) reported routine use of a nasogastric suction tube.
Heterogeneity was observed in the pancreatoduodenectomy practice patterns of surgeons in Brazil, some of them in contrast with established evidence in the literature.
胰十二指肠切除术是一项技术要求高的外科手术,术后并发症发生率在30%至61%之间。该手术需要高水平的经验,为将手术相关并发症和死亡率降至最低,高质量的标准手术势在必行。
了解巴西胰十二指肠切除术的手术实践模式。
设计了一份问卷,以获取胰腺癌手术实践、特定培训以及胰十二指肠切除术经验的概况。该调查发送给了表明对胰腺手术感兴趣的成员。
共发送了60份问卷,52份已返回(86.7%)。东南部的调查受访者最多,有25位外科医生(48.0%)。只有两位外科医生(3.9%)超过50%的胰十二指肠切除术通过腹腔镜进行。24位外科医生(46.2%)进行经典的惠普尔手术,43位外科医生(82.7%)进行标准的国际胰腺手术研究组淋巴结清扫术。重建方面,49位外科医生(94.2%)进行胰空肠吻合术,41位(78.9%)采用单肢技术,38位(73.1%)进行导管对黏膜吻合术,26位(50.0%)进行内部经吻合口支架置入,39位(75.0%)采用胃重建的结肠前途径,只有6位外科医生(11.5%)进行布朗肠肠吻合术。所有外科医生均进行预防性腹腔引流,6位外科医生(11.5%)使用生长抑素类似物。22位外科医生(42.3%)术后早期肠内营养为常规操作,34位外科医生(65.4%)报告常规使用鼻胃吸引管。
在巴西外科医生的胰十二指肠切除术实践模式中观察到异质性,其中一些与文献中的既定证据相反。