Purwar Sankalp, Venkataraman Ramesh, Senthilkumar R, Ramakrishnan Nagarajan, Abraham Babu K
Department of Critical Care Medicine, Apollo Hospitals, Chennai, Tamil Nadu, India.
Indian J Crit Care Med. 2014 Aug;18(8):503-7. doi: 10.4103/0972-5229.138147.
Use of noninvasive ventilation (NIV) outside guideline recommendations is common. We audited use of NIV in our tertiary care critical care unit (CCU) to evaluate appropriateness of use and patient outcomes when used outside level I recommendations.
Prospective observational study of all patients requiring NIV. Clinical parameters and arterial blood gases were recorded at initiation of NIV and 2 h later (or earlier if clinically warranted). NIV titration and decision to intubate were left to the discretion of treating intensivist. Patients were categorized into two groups: Group 1: Those with level I indications for use of NIV and group 2: All other levels of indications. Patients were followed until hospital discharge.
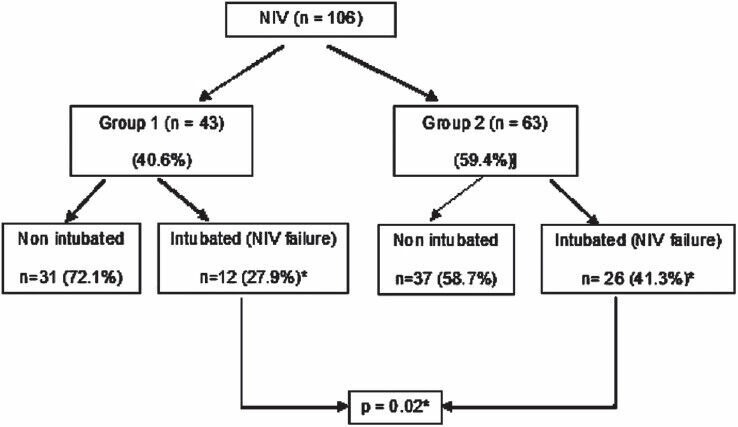
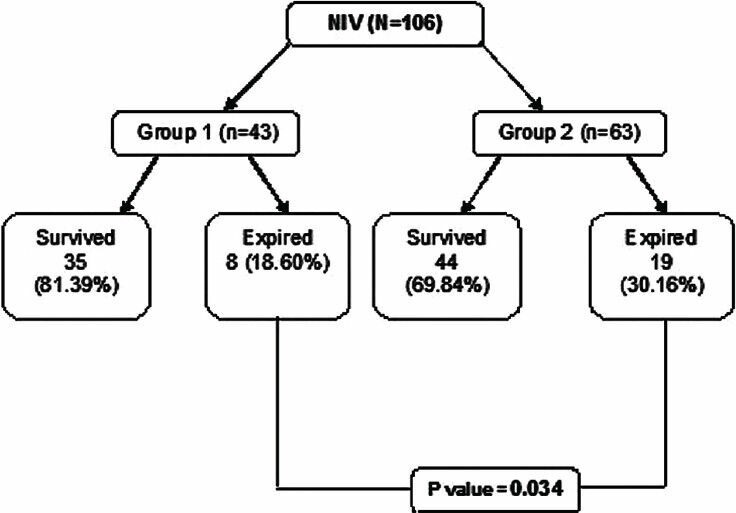
From January 2010 to June 2010, 1120 patients were admitted to the CCU. Of these 106 patients required NIV support with 40.6% (n = 43/106) being in group 1 and 59.4% (n = 63/106) in group 2. Of these 35.8% patients (38/106) failed NIV and required endotracheal intubation. NIV failure rates (41.27% vs. 27.91%; P = 0.02) and mortality (30.6% vs. 18.6%; P = 0.03) were significantly higher in group 2 patients. In a logistic regression analysis Acute Physiology and Chronic Health Evaluation (APACHE) II score (P = 0.02), time on NIV before intubation (P = 0.001) and baseline PaCO2 levels (P = 0.01) were strongly associated with mortality.
Noninvasive ventilation failure and mortality rates were significantly higher when used outside level I recommendations. APACHE II score, baseline PaCO2 and duration on NIV prior to intubation were predictors of increased mortality.
在指南推荐范围之外使用无创通气(NIV)的情况很常见。我们对三级医疗重症监护病房(CCU)中NIV的使用进行了审核,以评估在超出一级推荐范围使用时的使用合理性及患者预后。
对所有需要NIV的患者进行前瞻性观察研究。在开始NIV时及2小时后(或根据临床情况提前)记录临床参数和动脉血气。NIV滴定及插管决策由主治重症监护医生自行决定。患者分为两组:第1组:具有NIV一级使用指征的患者;第2组:所有其他指征水平的患者。对患者进行随访直至出院。
2010年1月至2010年6月,1120例患者入住CCU。其中106例患者需要NIV支持,第1组占40.6%(n = 43/106),第2组占59.4%(n = 63/106)。这些患者中35.8%(38/106)NIV治疗失败并需要气管插管。第2组患者的NIV失败率(41.27%对27.91%;P = 0.02)和死亡率(30.6%对18.6%;P = 0.03)显著更高。在逻辑回归分析中,急性生理与慢性健康状况评估(APACHE)II评分(P = 0.02)、插管前使用NIV的时间(P = 0.001)和基线PaCO2水平(P = 0.01)与死亡率密切相关。
在超出一级推荐范围使用时,无创通气失败率和死亡率显著更高。APACHE II评分、基线PaCO2以及插管前使用NIV的持续时间是死亡率增加的预测因素。