Denzler Annick, Burkhardt Tilo, Natalucci Giancarlo, Zimmermann Roland
Department of Obstetrics, Zurich University Hospital, Frauenklinikstraße 10, 8091 Zurich, Switzerland.
Department of Neonatology, Zurich University Hospital, Frauenklinikstraße 10, 8091 Zurich, Switzerland.
J Pregnancy. 2014;2014:874984. doi: 10.1155/2014/874984. Epub 2014 Jul 17.
To identify the risk factors for cystic periventricular leukomalacia (cPVL) and their implications for deciding between immediate delivery and conservative management of preterm prelabor rupture of the membranes (pPROM).
The following risk factors were compared between cPVL infants and 6440 controls: chorioamnionitis, sex, gestational age (GA), birth weight, pPROM, and pPROM-delivery interval. Factor impact on cPVL risk and clinical decision-making was determined by multivariate logistic regression.
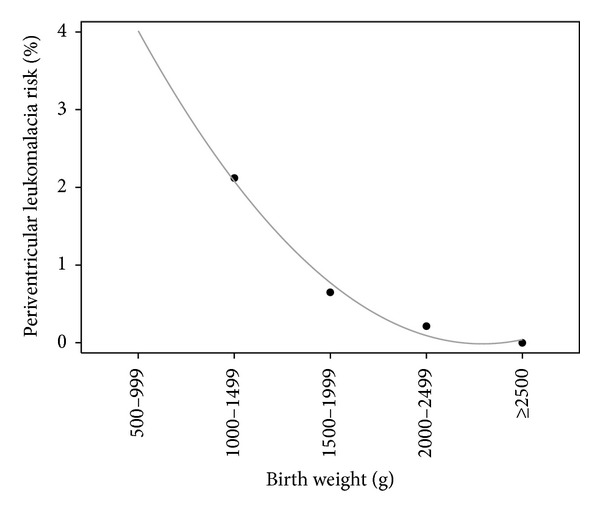
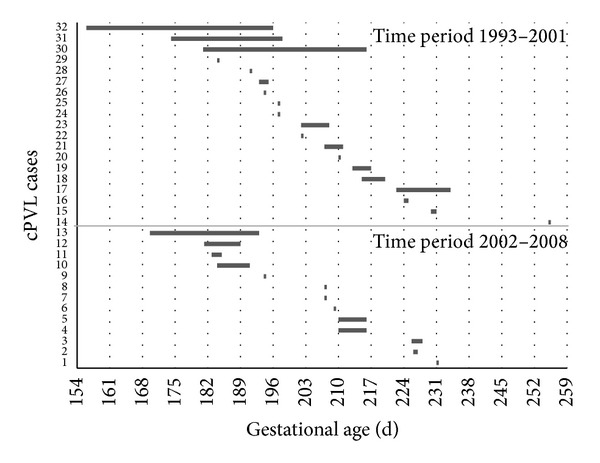
Overall cPVL prevalence (n = 32) was 0.99/1000 births. All cPVL infants but one were born <34 weeks of gestation and were <2500 g; 56% had histological chorioamnionitis versus 1.1% of controls (OR 35.9; 95%-CI 12.6-102.7). Because chorioamnionitis is a postnatal diagnosis, logistic regression was performed with prenatally available factors: pPROM-delivery interval >48 hours (OR 9.0; 95%-CI 4.1-20.0), male gender (OR 3.2; 95%-CI 1.4-7.3). GA was not a risk factor if birth weight was included. Risk decreased with increasing fetal weight despite a prolonged pPROM-delivery interval.
pPROM-delivery interval is the single most important prenatally available risk factor for the development of cPVL. Immediate delivery favors babies with chorioamnionitis but disfavors those with non infectious pPROM. In the absence of clinical chorioamnionitis fetal weight gain may offset the inflammatory risk of cPVL caused by a prolonged pPROM-delivery interval.
确定脑室周围白质软化症(cPVL)的危险因素及其对胎膜早破早产(pPROM)即刻分娩与保守治疗决策的影响。
比较cPVL婴儿与6440名对照者的以下危险因素:绒毛膜羊膜炎、性别、胎龄(GA)、出生体重、pPROM及pPROM至分娩间隔。通过多因素逻辑回归确定各因素对cPVL风险及临床决策的影响。
cPVL总体患病率(n = 32)为0.99/1000例分娩。除1例之外,所有cPVL婴儿均在孕34周前出生且体重<2500g;56%有组织学绒毛膜羊膜炎,而对照者为1.1%(比值比35.9;95%可信区间12.6 - 102.7)。由于绒毛膜羊膜炎为产后诊断,故采用产前可得因素进行逻辑回归分析:pPROM至分娩间隔>48小时(比值比9.0;95%可信区间4.1 - 20.0)、男性(比值比3.2;95%可信区间1.4 - 7.3)。若纳入出生体重,则胎龄不是危险因素。尽管pPROM至分娩间隔延长,但随着胎儿体重增加,风险降低。
pPROM至分娩间隔是产前可得的cPVL发生的最重要单一危险因素。即刻分娩对患绒毛膜羊膜炎的婴儿有利,但对非感染性pPROM的婴儿不利。在无临床绒毛膜羊膜炎的情况下,胎儿体重增加可能抵消pPROM至分娩间隔延长所致cPVL的炎症风险。