Saheb Sharif-Askari Fatemeh, Syed Sulaiman Syed Azhar, Saheb Sharif-Askari Narjes, Al Sayed Hussain Ali, Railey Mohammad Jaffar
School of Pharmacy, Universiti Sains Malaysia, Penang, Malaysia.
Pharmacy Department, Dubai Health Authority, Dubai, United Arab Emirates.
PLoS One. 2014 Sep 2;9(9):e106517. doi: 10.1371/journal.pone.0106517. eCollection 2014.
Anticoagulation therapy is usually required in patients with chronic kidney disease (CKD) for treatment or prevention of thromboembolic diseases. However, this benefit could easily be offset by the risk of bleeding.
To determine the incidence of adverse outcomes of anticoagulants in hospitalized patients with CKD, and to compare the rates of major bleeding events between the unfractionated heparin (UFH) and enoxaparin users.
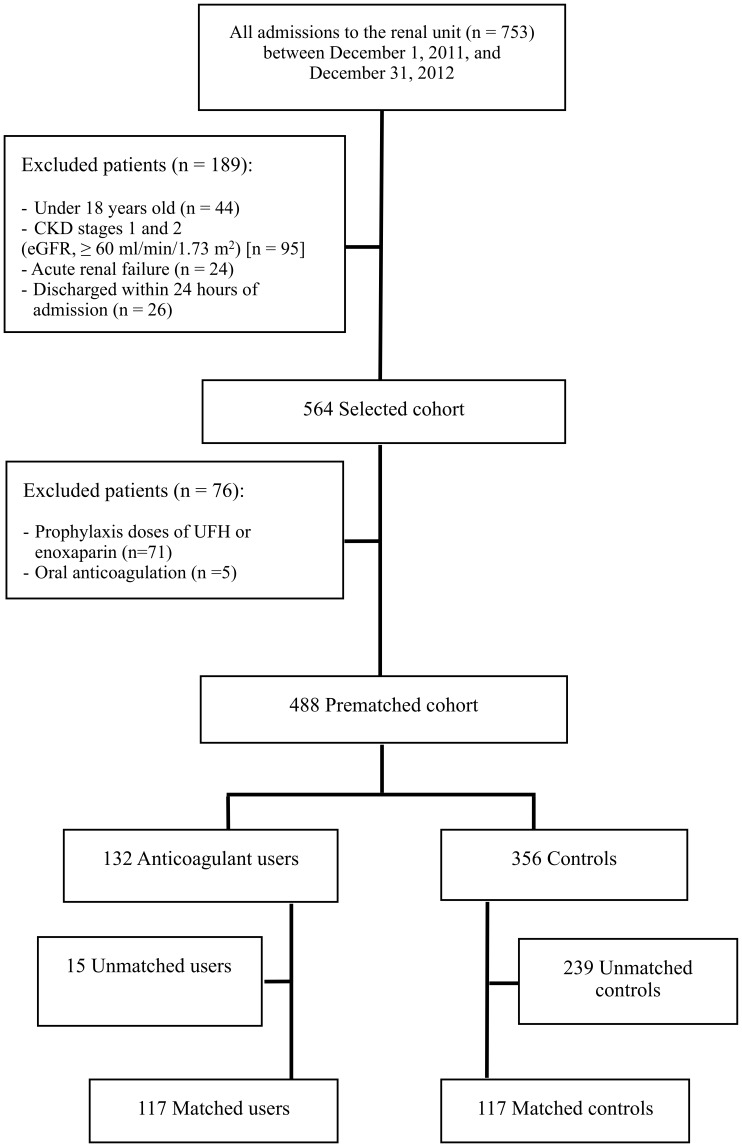
One year prospective observational study was conducted in patients with CKD stages 3 to 5 (estimated GFR, 10-59 ml/min/1.73 m(2)) who were admitted to the renal unit of Dubai Hospital. Propensity scores for the use of anticoagulants, estimated for each of the 488 patients, were used to identify a cohort of 117 pairs of patients. Cox regression method was used to estimate association between anticoagulant use and adverse outcomes.
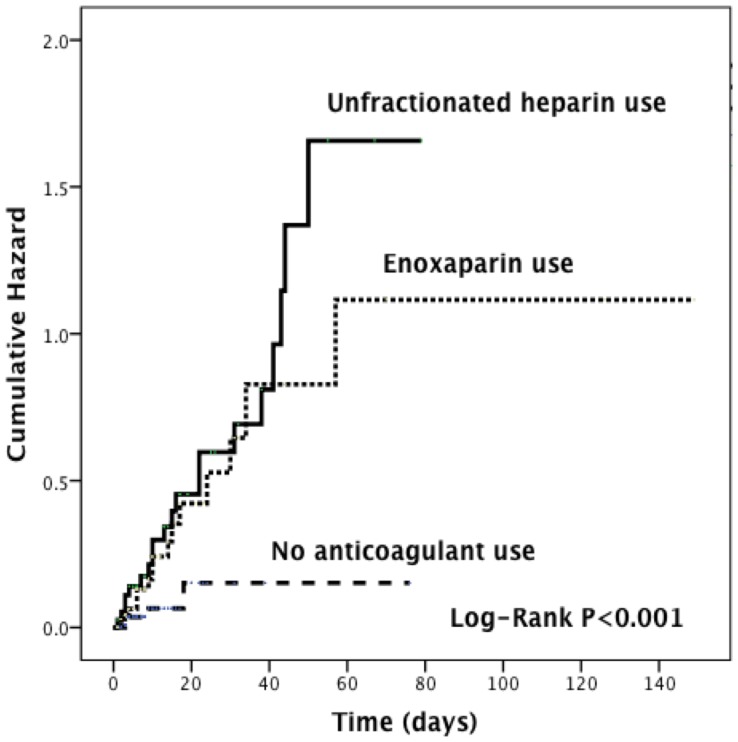
Major bleeding occurred in 1 in 3 patients who received anticoagulation during hospitalization (hazard ratio [HR], 4.61 [95% confidence interval [CI], 2.05-10.35]). Compared with enoxaparin users, patients who received anticoagulation with unfractionated heparin had a lower mean [SD] serum level of platelet counts (139.95 [113] × 10(3)/µL vs 205.56 [123] × 10(3)/µL; P<0.001), and had a higher risk of major bleeding (HR, 4.79 [95% CI, 1.85-12.36]). Furthermore, compared with those who did not receive anticoagulants, patients who did had a higher in-hospital mortality (HR, 2.54 [95% CI, 1.03-6.25]); longer length of hospitalization (HR, 1.04 [95% CI, 1.01-1.06]); and higher hospital readmission at 30 days (HR, 1.79 [95% CI, 1.10-2.91]).
Anticoagulation among hospitalized patients with CKD was significantly associated with an increased risk of bleeding and in-hospital mortality. Hence, intensive monitoring and preventive measures such as laboratory monitoring and/or dose adjustment are warranted.
慢性肾脏病(CKD)患者通常需要进行抗凝治疗以治疗或预防血栓栓塞性疾病。然而,这种益处很容易被出血风险所抵消。
确定住院CKD患者使用抗凝剂的不良结局发生率,并比较普通肝素(UFH)使用者和依诺肝素使用者的大出血事件发生率。
对入住迪拜医院肾内科的3至5期CKD患者(估计肾小球滤过率为10 - 59 ml/min/1.73 m²)进行了为期一年的前瞻性观察研究。为488例患者中的每一位估算了使用抗凝剂的倾向评分,以确定117对患者组成的队列。采用Cox回归方法估计抗凝剂使用与不良结局之间的关联。
住院期间接受抗凝治疗的患者中,每3人就有1人发生大出血(风险比[HR],4.61[95%置信区间[CI],2.05 - 10.35])。与依诺肝素使用者相比,接受普通肝素抗凝治疗的患者平均[标准差]血小板计数水平较低(139.95[113]×10³/µL对205.56[123]×10³/µL;P<0.001),且大出血风险较高(HR,4.79[95%CI,1.85 - 12.36])。此外,与未接受抗凝剂的患者相比,接受抗凝剂治疗的患者住院死亡率更高(HR,2.54[95%CI,1.03 - 6.25]);住院时间更长(HR,1.04[95%CI,1.01 - 1.06]);30天内再次入院率更高(HR,1.79[95%CI,1.10 - 2.91])。
住院CKD患者使用抗凝剂与出血风险和住院死亡率增加显著相关。因此,有必要进行强化监测并采取实验室监测和/或剂量调整等预防措施。