Manchester Institute of Nephrology and Transplantation, Manchester University NHS Foundation Trust, Oxford Road, Manchester, M13 9WL, UK.
Division of Pharmacy and Optometry, School of Health Sciences, The University of Manchester, Manchester Academic Health Science Centre, University of Manchester, Manchester, M13 9PT, UK.
J Nephrol. 2022 Nov;35(8):2015-2033. doi: 10.1007/s40620-022-01413-x. Epub 2022 Aug 25.
Patients with chronic kidney disease (CKD) have an increased risk of venous thromboembolism (VTE) and atrial fibrillation (AF). Anticoagulants have not been studied in randomised controlled trials with CrCl < 30 ml/min. The objective of this review was to identify the impact of different anticoagulant strategies in patients with advanced CKD including dialysis.
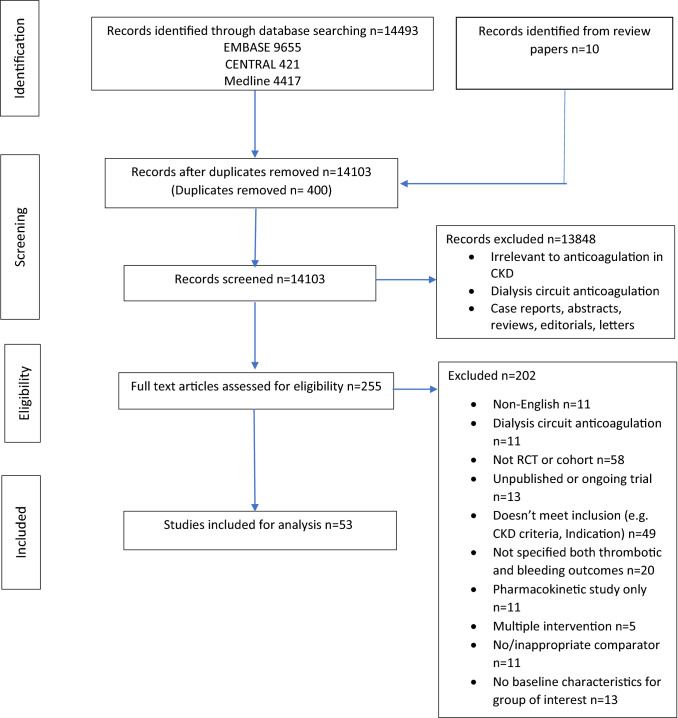
We conducted a systematic review of randomized controlled trials and cohort studies, searching electronic databases from 1946 to 2022. Studies that evaluated both thrombotic and bleeding outcomes with anticoagulant use in CrCl < 50 ml/min were included.
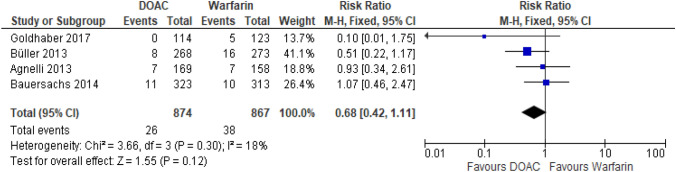
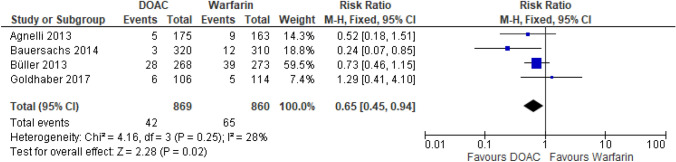
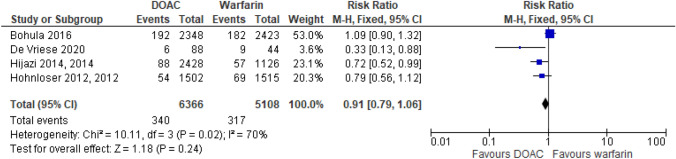
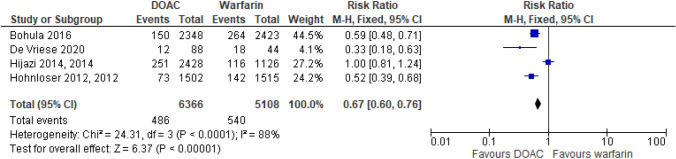
Our initial search yielded 14,503 papers with 53 suitable for inclusion. RCTs comparing direct oral anticoagulants (DOACs) versus warfarin for patients with VTE and CrCl 30-50 ml/min found no difference in recurrent VTE events (RR 0.68(95% CI 0.42-1.11)) with reduced bleeding (RR 0.65 (95% CI 0.45-0.94)). Observational data in haemodialysis suggest lower risk of recurrent VTE and major bleeding with apixaban versus warfarin. Very few studies examining outcomes were available for therapeutic and prophylactic dose low molecular weight heparin for CrCl < 30 ml/min. Findings for patients with AF on dialysis were that warfarin or DOACs had a similar or higher risk of stroke compared to no anticoagulation. For patients with AF and CrCl < 30 ml/min not on dialysis, anticoagulation should be considered on an individual basis, with limited studies suggesting DOACs may have a preferable safety profile.
Further studies are still required, some ongoing, in patients with advanced CKD (CrCl < 30 ml/min) to identify the safest and most effective treatment options for VTE and AF.
慢性肾脏病(CKD)患者发生静脉血栓栓塞症(VTE)和心房颤动(AF)的风险增加。尚未在 CrCl<30ml/min 的随机对照试验中研究过抗凝剂。本综述的目的是确定不同抗凝策略在包括透析在内的晚期 CKD 患者中的影响。
我们对随机对照试验和队列研究进行了系统评价,从 1946 年到 2022 年搜索电子数据库。纳入了评估 CrCl<50ml/min 时抗凝治疗与血栓栓塞和出血结局的研究。
我们最初的搜索产生了 14503 篇论文,其中 53 篇适合纳入。比较直接口服抗凝剂(DOACs)与华法林治疗 VTE 且 CrCl 为 30-50ml/min 的 RCT 发现,复发性 VTE 事件无差异(RR 0.68(95%CI 0.42-1.11)),出血减少(RR 0.65(95%CI 0.45-0.94))。血液透析中的观察性数据表明,阿哌沙班与华法林相比,VTE 复发和大出血的风险较低。对于 CrCl<30ml/min 的治疗和预防剂量低分子肝素,可用的研究结果很少。对于透析患者的 AF,与不抗凝相比,华法林或 DOACs 发生中风的风险更高或更高。对于未透析且 CrCl<30ml/min 的 AF 患者,应根据个体情况考虑抗凝治疗,一些研究表明 DOACs 的安全性可能更好。
仍需要进一步研究,一些正在进行的研究,以确定晚期 CKD(CrCl<30ml/min)患者 VTE 和 AF 最安全和最有效的治疗选择。