Kaguthi G, Nduba V, Nyokabi J, Onchiri F, Gie R, Borgdorff M
Kenya Medical Research Institute, Centre for Respiratory Diseases Research (CRDR), Kisumu, Nairobi 40100, Kenya.
Kenya Medical Research Institute, Centre for Respiratory Diseases Research (CRDR), Kisumu, Nairobi 40100, Kenya ; Academic Medical Centre (AMC), University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
Interdiscip Perspect Infect Dis. 2014;2014:291841. doi: 10.1155/2014/291841. Epub 2014 Aug 17.
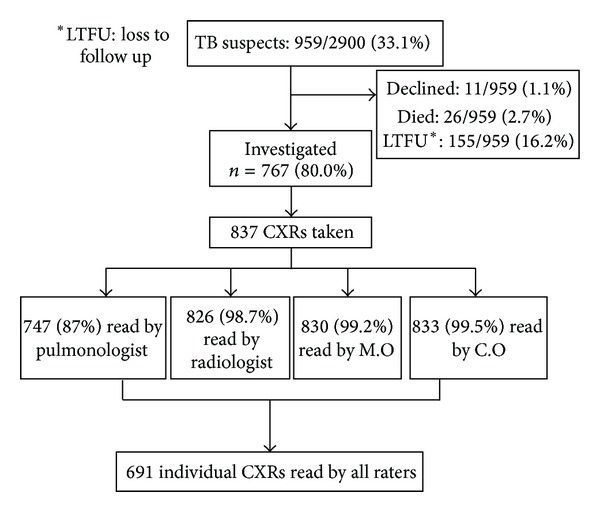
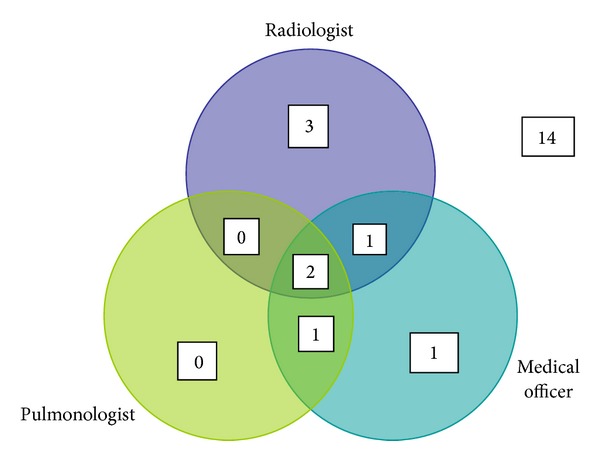
The chest radiograph (CXR) is considered a key diagnostic tool for pediatric tuberculosis (TB) in clinical management and endpoint determination in TB vaccine trials. We set out to compare interrater agreement for TB diagnosis in western Kenya. A pediatric pulmonologist and radiologist (experts), a medical officer (M.O), and four clinical officers (C.Os) with basic training in pediatric CXR reading blindly assessed CXRs of infants who were TB suspects in a cohort study. C.Os had access to clinical findings for patient management. Weighted kappa scores summarized interrater agreement on lymphadenopathy and abnormalities consistent with TB. Sensitivity and specificity of raters were determined using microbiologically confirmed TB as the gold standard (n = 8). A total of 691 radiographs were reviewed. Agreement on abnormalities consistent with TB was poor; k = 0.14 (95% CI: 0.10-0.18) and on lymphadenopathy moderate k = 0.26 (95% CI: 0.18-0.36). M.O [75% (95% CI: 34.9%-96.8%)] and C.Os [63% (95% CI: 24.5%-91.5%)] had high sensitivity for culture confirmed TB. TB vaccine trials utilizing expert agreement on CXR as a nonmicrobiologically confirmed endpoint will have reduced specificity and will underestimate vaccine efficacy. C.Os detected many of the bacteriologically confirmed cases; however, this must be interpreted cautiously as they were unblinded to clinical features.
胸部X光片(CXR)在儿童结核病(TB)的临床管理和TB疫苗试验的终点判定中被视为关键的诊断工具。我们着手比较肯尼亚西部TB诊断的不同评估者之间的一致性。在一项队列研究中,一名儿科肺科医生和一名放射科医生(专家)、一名医务官员(M.O)以及四名接受过儿科CXR阅片基础培训的临床官员(C.Os)对TB疑似婴儿的CXR进行了盲法评估。C.Os可获取用于患者管理的临床检查结果。加权kappa评分总结了不同评估者在淋巴结病和与TB相符的异常方面的一致性。以微生物学确诊的TB作为金标准(n = 8)来确定评估者的敏感性和特异性。共审查了691张X光片。在与TB相符的异常方面一致性较差;kappa值 = 0.14(95%可信区间:0.10 - 0.18),在淋巴结病方面一致性中等,kappa值 = 0.26(95%可信区间:0.18 - 0.36)。M.O [75%(95%可信区间:34.9% - 96.8%)] 和C.Os [63%(95%可信区间:24.5% - 91.5%)] 对培养确诊的TB具有较高的敏感性。利用专家对CXR的一致性作为非微生物学确诊终点的TB疫苗试验将降低特异性,并会低估疫苗效力。C.Os检测出了许多细菌学确诊病例;然而,由于他们知晓临床特征,所以对此必须谨慎解读。