Liu Xiaosun, Jin Hailong, Zhang Geer, Lin Xianke, Chen Chao, Sun Jianyi, Zhang Yu, Zhang Qing, Yu Jiren
Department of Gastrointestinal Surgery, the First Affiliated Hospital, Medical College, Zhejiang University, Hangzhou, China.
PLoS One. 2014 Sep 8;9(9):e106834. doi: 10.1371/journal.pone.0106834. eCollection 2014.
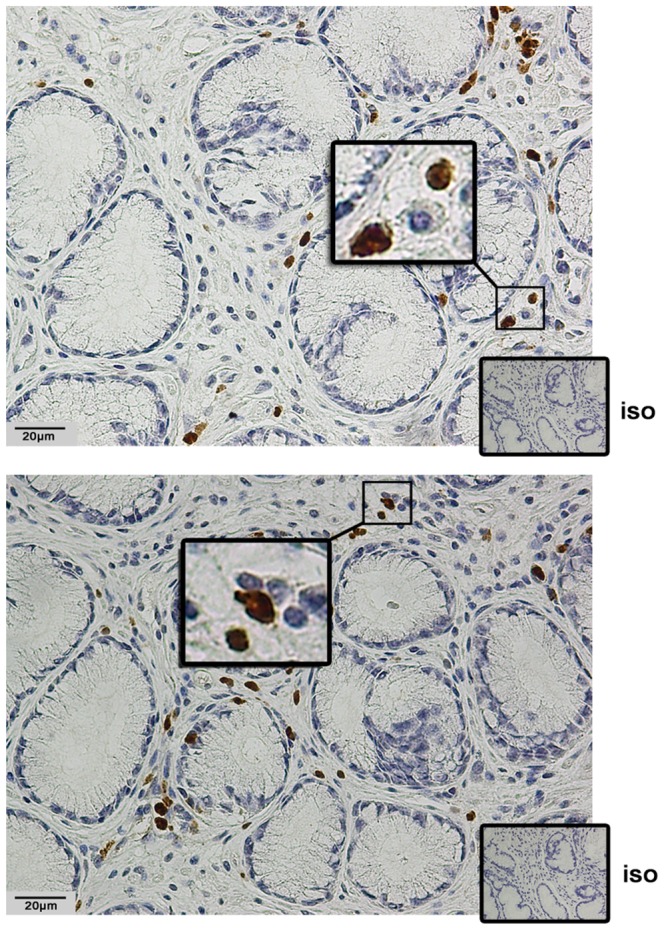
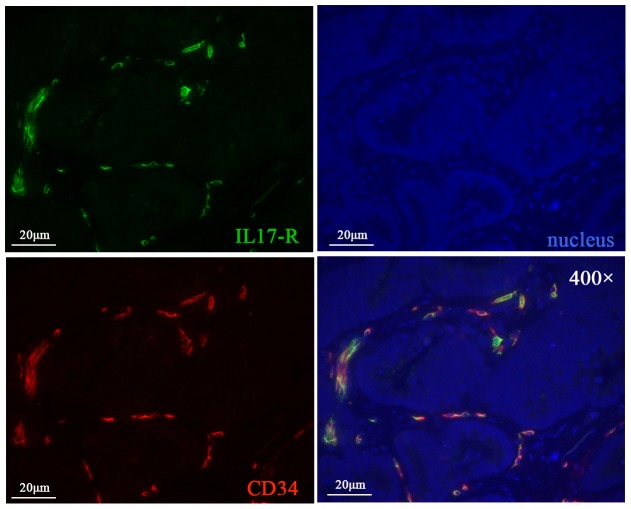
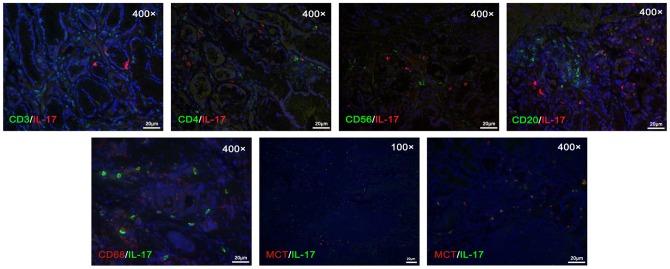
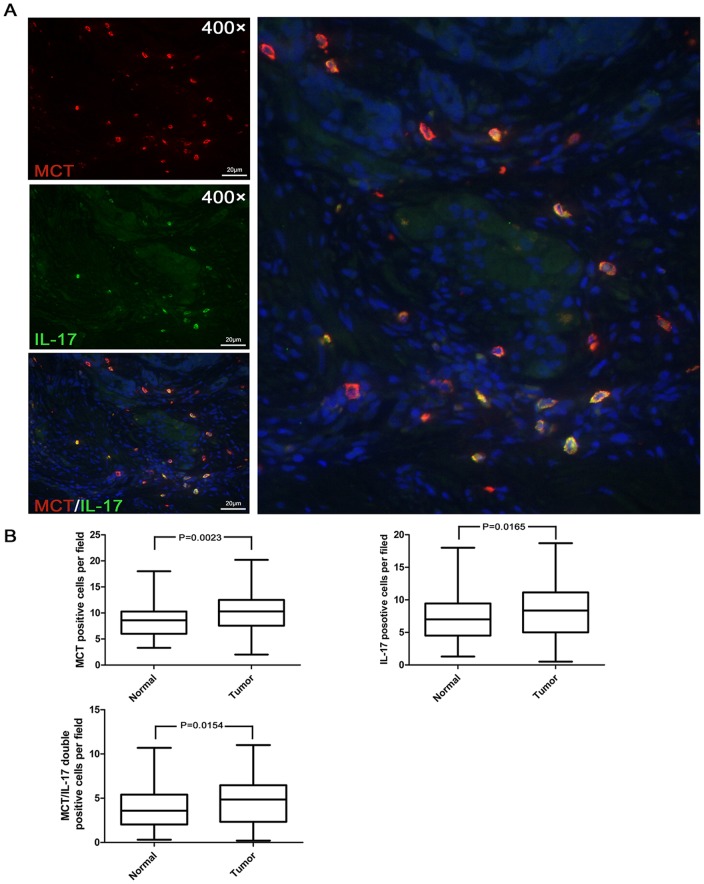
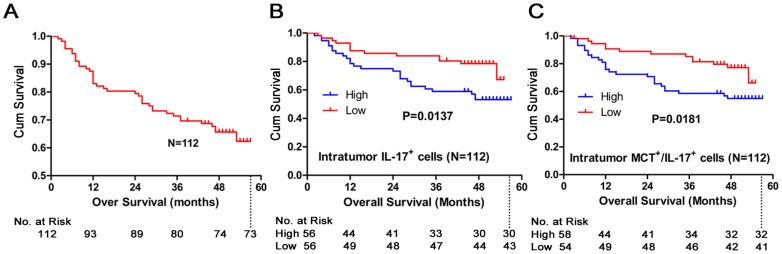
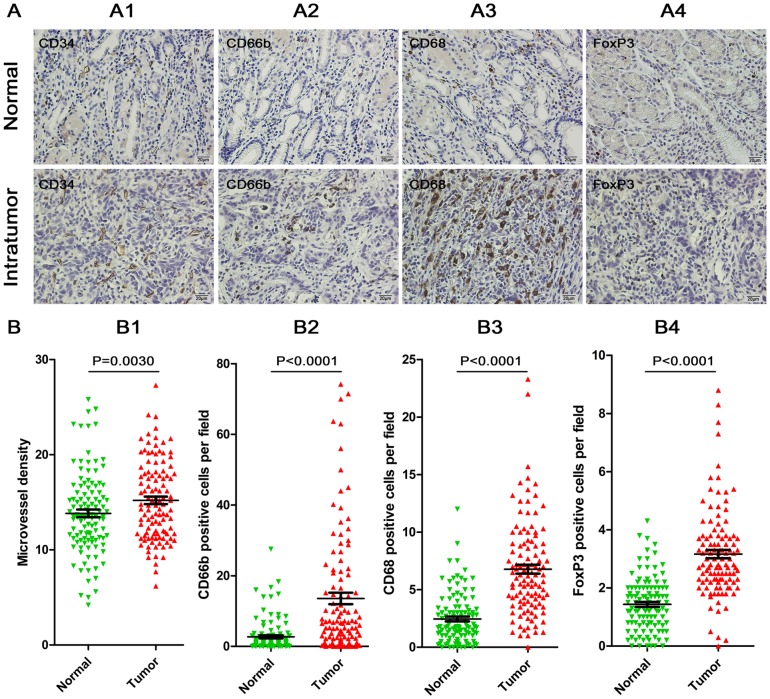
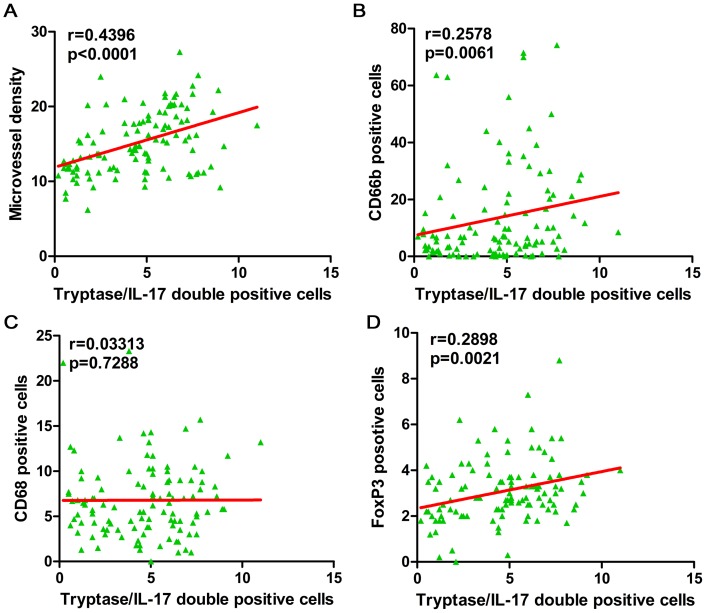
Interleukin-17 (IL-17) is prevalent in tumor tissue and suppresses effective anti-tumor immune responses. However, the source of the increased tumor-infiltrating IL-17 and its contribution to tumor progression in human gastric cancer remain poorly understood. In this study, we enrolled 112 gastric cancer patients, immunofluorescence was used to evaluate the colocalization of CD3, CD4, CD56, CD20, CD68, and mast cell tryptase (MCT) with IL-17. Immunohistochemistry was used to evaluate the distribution of microvessel density (CD34), CD66b(+), CD68(+), and FoxP3(+) cells in different microanatomical areas. Prognostic value was determined by Kaplan-Meier analysis and a Cox regression model. The results showed that mast cells, but not T cells or macrophages, were the predominant cell type producing IL-17 in gastric cancer. Significant positive correlations were detected between densities of mast cell-derived IL-17 and microvessels, neutrophils, and regulatory T cells (Tregs). Furthermore, we found that the majority of vascular endothelial cells expressing Interleukin-17 receptor (IL-17R). Kaplan-Meier analysis revealed that increasing intratumor infiltrated mast cells and IL-17(+) cells, as well as MCT(+) IL-17(+) cells, were significantly associated with worse overall survival. These findings indicated that mast cells were the major source of IL-17 in gastric cancer, and intratumor IL-17 infiltration may have promoted tumor progression by enhancing angiogenesis in the tumor microenvironment through the axis of IL-17/IL-17R. IL-17-positive mast cells showed a prognostic factor in gastric cancer, indicating that immunotherapy targeting mast cells might be an effective strategy to control intratumor IL-17 infiltration, and consequently reverse immunosuppression in the tumor microenvironment, facilitating cancer immunotherapy.
白细胞介素-17(IL-17)在肿瘤组织中普遍存在,并抑制有效的抗肿瘤免疫反应。然而,肿瘤浸润性IL-17增加的来源及其对人类胃癌肿瘤进展的贡献仍知之甚少。在本研究中,我们招募了112例胃癌患者,采用免疫荧光法评估CD3、CD4、CD56、CD20、CD68和肥大细胞类胰蛋白酶(MCT)与IL-17的共定位。采用免疫组织化学法评估不同微解剖区域微血管密度(CD34)、CD66b(+)、CD68(+)和FoxP3(+)细胞的分布。通过Kaplan-Meier分析和Cox回归模型确定预后价值。结果显示,肥大细胞而非T细胞或巨噬细胞是胃癌中产生IL-17的主要细胞类型。在肥大细胞来源的IL-17密度与微血管、中性粒细胞和调节性T细胞(Tregs)之间检测到显著正相关。此外,我们发现大多数血管内皮细胞表达白细胞介素-17受体(IL-17R)。Kaplan-Meier分析显示,肿瘤内浸润的肥大细胞和IL-17(+)细胞以及MCT(+)IL-17(+)细胞增加与总体生存率较差显著相关。这些发现表明,肥大细胞是胃癌中IL-17的主要来源,肿瘤内IL-17浸润可能通过IL-17/IL-17R轴增强肿瘤微环境中的血管生成,从而促进肿瘤进展。IL-17阳性肥大细胞是胃癌的一个预后因素,表明靶向肥大细胞的免疫治疗可能是控制肿瘤内IL-17浸润的有效策略,从而逆转肿瘤微环境中的免疫抑制,促进癌症免疫治疗。