Cook Elizabeth A, Schneider Kathleen M, Robinson Jennifer, Wilwert June, Chrischilles Elizabeth, Pendergast Jane, Brooks John
University of Iowa College of Pharmacy, Iowa City, IA, USA.
BMC Health Serv Res. 2014 Sep 15;14:391. doi: 10.1186/1472-6963-14-391.
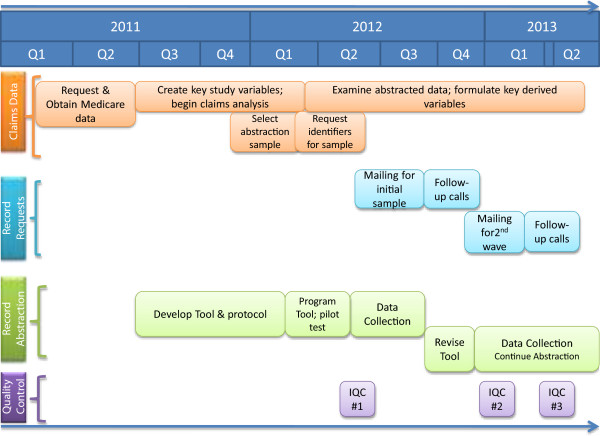
Comparative effectiveness studies using Medicare claims data are vulnerable to treatment selection biases and supplemental data from a sample of patients has been recommended for examining the magnitude of this bias. Previous research using nationwide Medicare claims data has typically relied on the Medicare Current Beneficiary Survey (MCBS) for supplemental data. Because many important clinical variables for our specific research question are not available in the MCBS, we collected medical record data from a subsample of patients to assess the validity of assumptions and to aid in the interpretation of our estimates. This paper seeks to describe and document the process used to collect and validate this supplemental information.
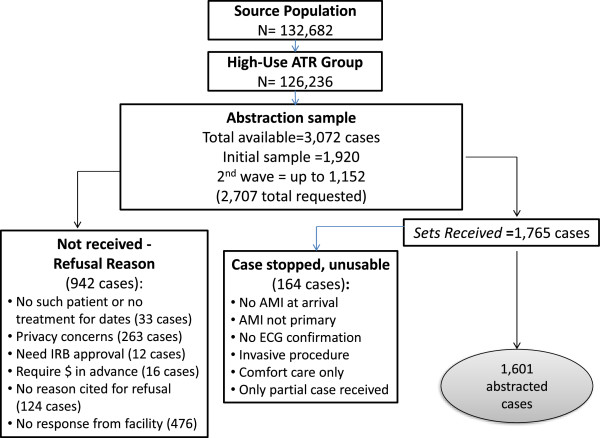
Medicare claims data files for all patients with fee-for-service Medicare benefits who had an acute myocardial infarction (AMI) in 2007 or 2008 were obtained. Medical records were obtained and abstracted for a stratified subsample of 1,601 of these patients, using strata defined by claims-based measures of physician prescribing practices and drug treatment combinations. The abstraction tool was developed collaboratively by study clinicians and researchers, leveraging important elements from previously validated tools.
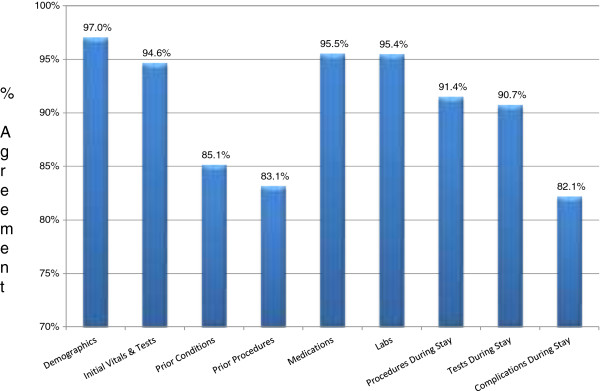
Records for 2,707 AMI patients were requested from the admitting hospitals and 1,751 were received for an overall response rate of 65%; 1,601 cases were abstracted by trained personnel at a contracted firm. Data were collected with overall 96% inter-abstractor agreement across all variables. Some non-response bias was detected at the patient and facility level.
Although Medicare claims data are a potentially powerful resource for conducting comparative effectiveness analyses, observational databases are vulnerable to treatment selection biases. This study demonstrates that it is feasible to abstract medical records for Medicare patients nationwide and collect high quality data, to design the sampling purposively to address specific research questions, and to more thoroughly evaluate the appropriateness of care delivered to AMI patients.
利用医疗保险索赔数据进行的比较有效性研究容易受到治疗选择偏倚的影响,有人建议使用患者样本的补充数据来检验这种偏倚的程度。以往使用全国医疗保险索赔数据的研究通常依赖医疗保险当前受益人调查(MCBS)作为补充数据。由于我们特定研究问题的许多重要临床变量在MCBS中不可用,我们从患者子样本中收集了病历数据,以评估假设的有效性并帮助解释我们的估计值。本文旨在描述和记录用于收集和验证这些补充信息的过程。
获取了2007年或2008年患有急性心肌梗死(AMI)的所有享受按服务付费医疗保险福利患者的医疗保险索赔数据文件。使用基于索赔的医生处方实践和药物治疗组合测量方法定义的分层,从这些患者的1601个分层子样本中获取并提取病历。抽象工具由研究临床医生和研究人员共同开发,借鉴了先前经过验证的工具中的重要元素。
向收治医院索要了2707例AMI患者的记录,收到了1751例,总体回复率为65%;1601例由一家签约公司的经过培训的人员进行了提取。所有变量的总体抽取者间一致性为96%。在患者和机构层面检测到了一些无应答偏倚。
尽管医疗保险索赔数据是进行比较有效性分析的潜在强大资源,但观察性数据库容易受到治疗选择偏倚的影响。本研究表明,对全国医疗保险患者的病历进行提取并收集高质量数据、有目的地设计抽样以解决特定研究问题以及更全面地评估为AMI患者提供的护理的适宜性是可行的。