Janssen Paddy Kc, Touw Daan, Schweitzer Dave H, Waldinger Marcel D
Division of Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Faculty of BetaSciences, Utrecht University, Utrecht, The Netherlands. ; Department of Central Hospital Pharmacy, Viecuri Hospital, Venlo, The Netherlands.
Apotheek Haagse Ziekenhuizen, HagaZiekenhuis, Den Haag, The Netherlands.
Korean J Urol. 2014 Sep;55(9):599-607. doi: 10.4111/kju.2014.55.9.599. Epub 2014 Sep 5.
Nonresponse to any selective serotonin reuptake inhibitor (SSRI) treatment is rare. In this study, we aimed to investigate ejaculation delay nonresponse to paroxetine treatment in men with lifelong premature ejaculation (PE) who were also known to be nonresponders to other SSRIs.
Five males with lifelong PE who were known nonresponders to paroxetine and other serotonergic antidepressants and eight males with lifelong PE who were specifically recruited were included. Blood sampling occurred 1 month and 1 day before the start of treatment and at the end of three consecutive series of 4 weeks of daily treatment with 10-, 20-, and 30-mg paroxetine, respectively. Blood samples for measurement of leptin and paroxetine were taken at 8:30 AM, 9:30 AM, 10:30 AM, and 11:30 AM, respectively. At 9:00 AM, one tablet of 10-, 20-, or 30-mg paroxetine was taken during the first, second, and third month, respectively. Intravaginal ejaculatory latency time (IELT) was measured with a stopwatch. The main outcome measures were the fold increase in the geometric mean IELT, serum leptin and paroxetine concentrations, body mass index (BMI), 5-HT1A receptor C-1019G polymorphism, and CYP2D6 mutations.
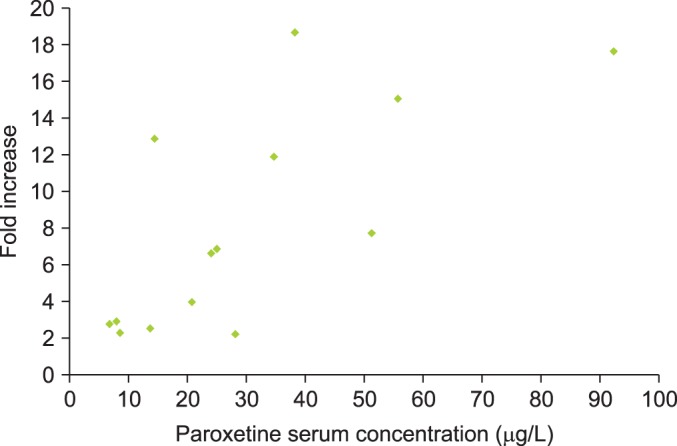
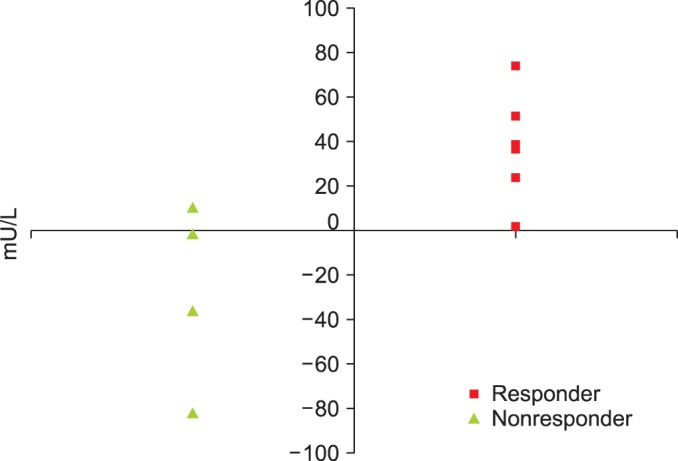
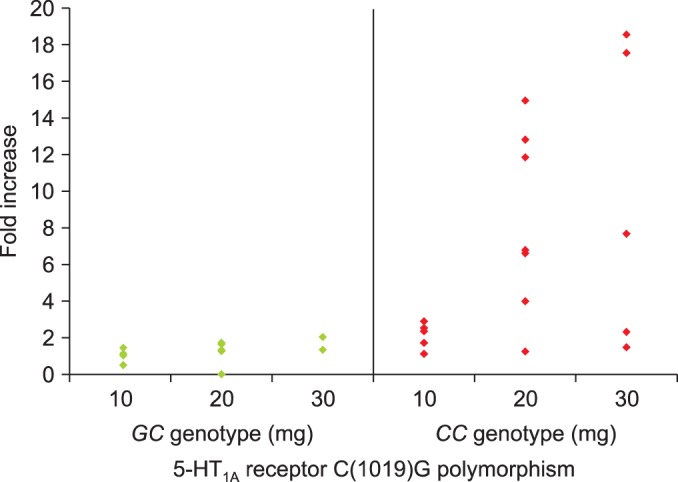
Between the 7 paroxetine responders and 6 nonresponders, the fold increase in the geometric mean IELT was significantly different after daily 10-mg (p=0.003), 20-mg (p=0.002), and 30-mg paroxetine (p=0.026) and ranged from 2.0 to 8.8 and from 1.1 to 1.7, respectively. BMI at baseline and at the end of the study was not significantly different between responders and nonresponders. Serum leptin levels at baseline were similar in responders and nonresponders and did not change during treatment. The serum paroxetine concentration increased with increasing dosage and was not significantly different between responders and nonresponders. There was no association between the fold increase in the geometric mean IELT and serum paroxetine levels during the three treatment periods nor between leptin levels during the treatment periods and serum paroxetine levels. For the 5-HT1A receptor C-1019G variation, all responders had the CC genotype and all nonresponders had the GC genotype, respectively.
Complete absence of paroxetine-induced ejaculation delay is presumably related to pharmacodynamic factors and perhaps to 5-HT1A receptor gene polymorphism.
对任何选择性5-羟色胺再摄取抑制剂(SSRI)治疗无反应的情况很罕见。在本研究中,我们旨在调查终身早泄(PE)且已知对其他SSRI无反应的男性对帕罗西汀治疗射精延迟无反应的情况。
纳入5名已知对帕罗西汀和其他血清素能抗抑郁药无反应的终身PE男性,以及8名专门招募的终身PE男性。在治疗开始前1个月零1天以及分别用10毫克、20毫克和30毫克帕罗西汀进行连续三个4周疗程治疗结束时进行采血。分别在上午8:30、9:30、10:30和11:30采集用于测量瘦素和帕罗西汀的血样。在第一个月、第二个月和第三个月的上午9:00,分别服用一片10毫克、20毫克或30毫克的帕罗西汀。用秒表测量阴道内射精潜伏期(IELT)。主要观察指标为几何平均IELT的增加倍数、血清瘦素和帕罗西汀浓度、体重指数(BMI)、5-HT1A受体C-1019G多态性以及CYP2D6突变。
在7名帕罗西汀反应者和6名无反应者之间,每日服用10毫克(p = 0.003)、20毫克(p = 0.002)和30毫克帕罗西汀(p = 0.026)后,几何平均IELT的增加倍数有显著差异,分别为2.0至8.8和1.1至1.7。反应者和无反应者在基线和研究结束时的BMI无显著差异。反应者和无反应者的基线血清瘦素水平相似,且治疗期间未发生变化。血清帕罗西汀浓度随剂量增加而升高,反应者和无反应者之间无显著差异。在三个治疗期内,几何平均IELT的增加倍数与血清帕罗西汀水平之间,以及治疗期内的瘦素水平与血清帕罗西汀水平之间均无关联。对于5-HT1A受体C-1019G变异,所有反应者分别具有CC基因型,所有无反应者分别具有GC基因型。
帕罗西汀诱导的射精延迟完全缺失可能与药效学因素有关,或许还与5-HT1A受体基因多态性有关。