Maretty-Nielsen Katja, Aggerholm-Pedersen Ninna, Keller Johnny, Safwat Akmal, Baerentzen Steen, Pedersen Alma B
Sarcoma Centre of Aarhus University Hospital, Aarhus, Denmark.
BMC Cancer. 2014 Sep 19;14:682. doi: 10.1186/1471-2407-14-682.
Cancer-specific survival estimates rely on precise and correct data on the cause of death; however, these data can be difficult to acquire, particularly in elderly patients where comorbidity is common. Furthermore, while some deaths are directly related to cancer, others are more complex, with cancer merely contributing. Another, more precise, method is to assess the relative mortality, i.e., mortality in patients compared to the general population. The aims of this study were to describe the relative mortality in soft tissue sarcoma, and to compare the relative mortality with the cancer-specific mortality.
We included 1246 patients treated for soft tissue sarcoma and 6230 individually age- and sex-matched individuals from the general population. The relative mortality was estimated as rates, and rate ratios adjusted for comorbidity. Mortality rate ratios were computed using the Cox proportional hazard model for 0-5 years and 5-10 years, according to age, sex and level of comorbidity. The cancer-specific mortality was compared to the corresponding relative mortality.
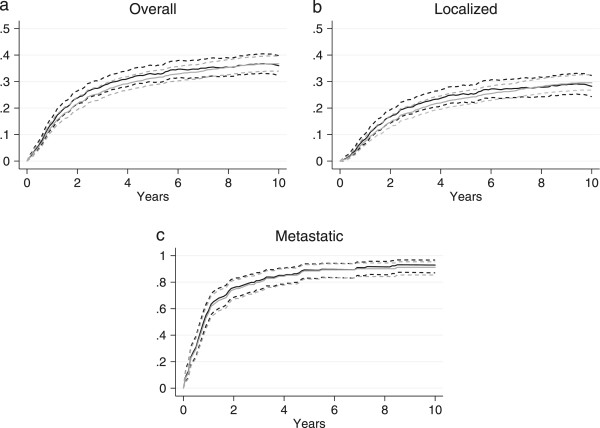
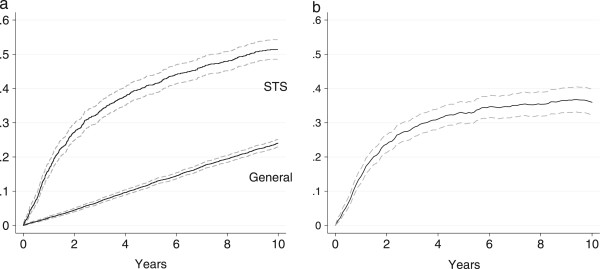
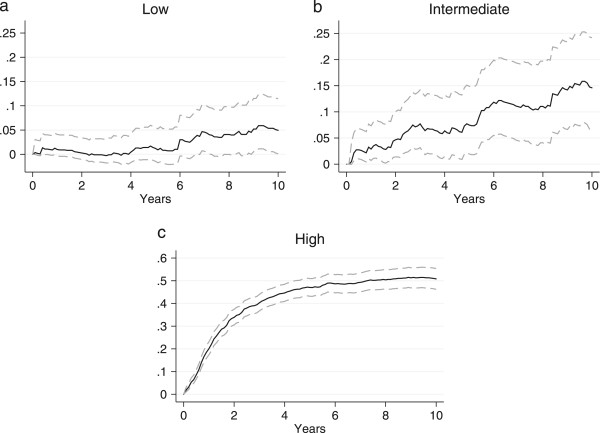
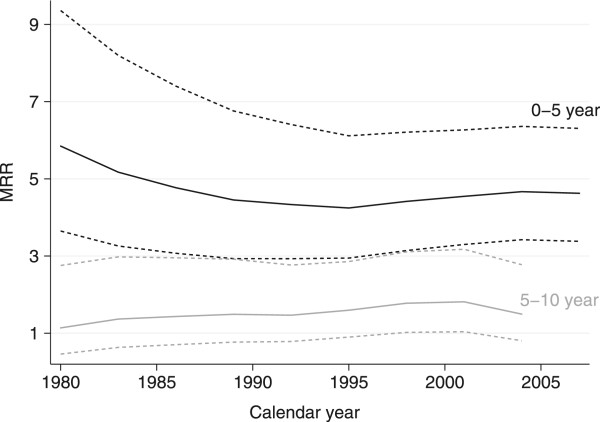
The overall 5- and 10-year relative mortality was 32.8% and 36.0%. Patients with low-grade soft tissue sarcoma did not have increased mortality compared with the general population. Soft tissue sarcoma patients had a 4.4 times higher risk of dying within the first five years after diagnosis and a 1.6 times higher risk between five and ten years compared with the general comparison cohort. The relative mortality varied according to age, grade, stage at diagnosis, and level of comorbidity, being highest in younger patients and in patients without comorbidity. The overall 5- and 10-year cancer-specific mortality was underestimated by 1.5 and overestimated by 0.7 percentage points compared to the relative mortality, respectively. No statistical significant difference between the relative and the cancer-specific mortality was found.
The relative mortality provides an unbiased and accurate method to differentiate between cancer-specific and non-cancer-specific deaths. However, when data on the cause of death is of a sufficient quality, there is no difference between relative mortality and disease-specific mortality based on death certificates.
癌症特异性生存估计依赖于关于死亡原因的精确且正确的数据;然而,这些数据可能难以获取,尤其是在合并症常见的老年患者中。此外,虽然一些死亡与癌症直接相关,但其他死亡情况更为复杂,癌症只是其中一个因素。另一种更精确的方法是评估相对死亡率,即患者与一般人群相比的死亡率。本研究的目的是描述软组织肉瘤的相对死亡率,并将相对死亡率与癌症特异性死亡率进行比较。
我们纳入了1246例接受软组织肉瘤治疗的患者以及6230例来自一般人群的按年龄和性别个体匹配的个体。相对死亡率以比率估计,并对合并症进行了比率调整。根据年龄、性别和合并症水平,使用Cox比例风险模型计算0至5年和5至10年的死亡率比率。将癌症特异性死亡率与相应的相对死亡率进行比较。
总体5年和10年相对死亡率分别为32.8%和36.0%。低级别软组织肉瘤患者与一般人群相比死亡率没有增加。与一般对照队列相比,软组织肉瘤患者在诊断后的前五年内死亡风险高4.4倍,在五年至十年间死亡风险高1.6倍。相对死亡率因年龄、分级、诊断时的分期和合并症水平而异,在年轻患者和无合并症患者中最高。总体5年和10年癌症特异性死亡率分别比相对死亡率低估1.5个百分点和高估0.7个百分点。相对死亡率与癌症特异性死亡率之间未发现统计学显著差异。
相对死亡率提供了一种无偏且准确的方法来区分癌症特异性死亡和非癌症特异性死亡。然而,当死亡原因数据质量足够时,基于死亡证明的相对死亡率和疾病特异性死亡率之间没有差异。