Driscoll Andrea, Srivastava Piyush, Toia Deidre, Gibcus Jackie, Hare David L
School of Nursing and Midwifery, Deakin University, 225 Burwood Highway, Melbourne, Burwood, Australia.
BMC Res Notes. 2014 Sep 23;7:668. doi: 10.1186/1756-0500-7-668.
Beta-adrenergic blockade has been shown to improve left ventricular function, reduce hospital admissions and improve survival in chronic heart failure with reduced ejection fraction (HFrEF), with mortality reduction starting early after beta-adrenergic receptor blocker initiation and being dose-related. The aim of this pilot study was to determine the effectiveness of a nurse-led titration clinic in improving the time required for patients to reach optimal doses of the beta-adrenergic receptor blocking agents.
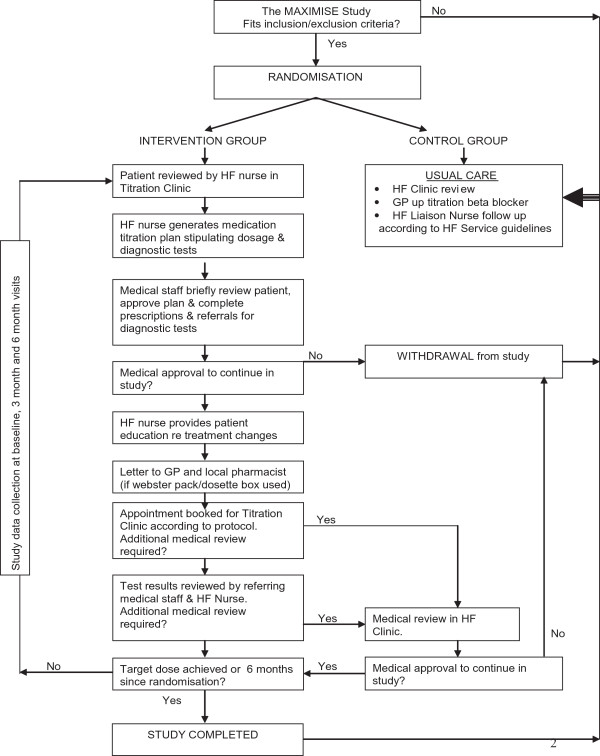
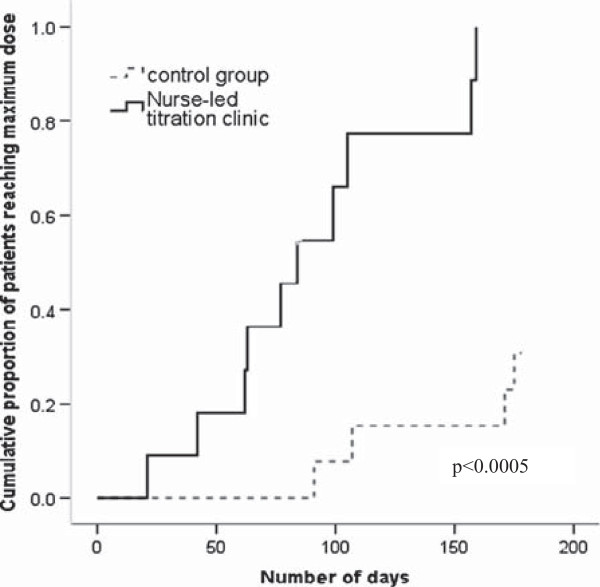
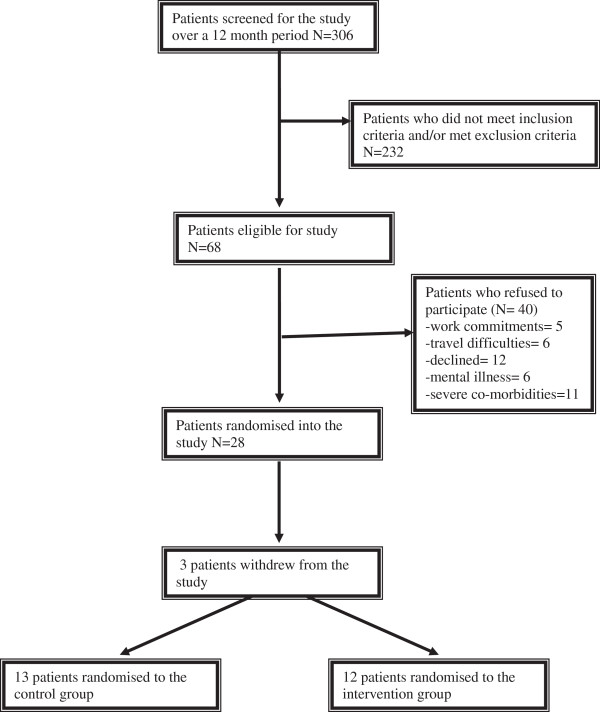
We conducted a prospective pilot randomized controlled trial. Twenty eight patients with CHF were randomized to optimisation of beta-adrenergic receptor blocker therapy over six months by either a nurse-led titration (NLT) clinic, led by a nurse specialist with the support of a cardiologist in a CHF clinic, or by their primary care physician (usual care (UC)). The primary endpoint was time to maximal beta-adrenergic receptor blocker dose. The secondary end-point was the proportion of patients reaching the target dose of beta-adrenergic receptor blocker by six months.
The patients were predominantly men (72%), age 67 ± 16 years; New York Heart Association (NYHA) functional class I (32%), II (44%) and III (20%); baseline left ventricular ejection fraction 33 ± 10%, and a low mean Charlson co-morbidity score of 2.5 ± 1.4. The time to maximum dose was shorter in the NLT group compared to the UC group (90 ± 14 vs 166 ± 8 days, p < 0.0005). At six months, in the NLT group there were nine patients (82%) on high dose and one patient (9%) on low dose beta-adrenergic receptor blocker compared to the UC group with five (42%) patients reaching maximum dose and five (42%) patients on low dose (p = 0.04). The patients allocated to the NLT group also had significantly less worsening of depression between baseline and six months (p = 0.006).
A NLT clinic improves optimisation of beta-adrenergic receptor blocker therapy through increasing the proportion of patients reaching maximal dose and facilitating rapid up-titration of beta-adrenergic receptor blocker agents in patients with chronic HFrEF.
Australian Clinical Trials Registry (ACTRN012606000383561).
β-肾上腺素能阻滞剂已被证明可改善左心室功能,减少慢性射血分数降低的心力衰竭(HFrEF)患者的住院次数并提高生存率,β-肾上腺素能受体阻滞剂开始使用后早期死亡率即开始降低,且与剂量相关。这项初步研究的目的是确定护士主导的滴定门诊在缩短患者达到β-肾上腺素能受体阻滞剂最佳剂量所需时间方面的有效性。
我们进行了一项前瞻性初步随机对照试验。28例CHF患者被随机分为两组,一组通过由护士专家主导、心脏病专家在CHF门诊提供支持的护士主导滴定(NLT)门诊,另一组由其初级保健医生(常规治疗(UC)),在六个月内优化β-肾上腺素能受体阻滞剂治疗。主要终点是达到最大β-肾上腺素能受体阻滞剂剂量的时间。次要终点是六个月内达到β-肾上腺素能受体阻滞剂目标剂量的患者比例。
患者主要为男性(72%),年龄67±16岁;纽约心脏协会(NYHA)心功能分级Ⅰ级(32%)、Ⅱ级(44%)和Ⅲ级(20%);基线左心室射血分数33±10%,平均Charlson合并症评分较低,为2.5±1.4。与UC组相比,NLT组达到最大剂量的时间更短(90±14天对166±8天,p<0.0005)。六个月时,NLT组有9例患者(82%)使用高剂量β-肾上腺素能受体阻滞剂,1例患者(9%)使用低剂量,而UC组有5例患者(42%)达到最大剂量,5例患者(42%)使用低剂量(p=0.04)。分配到NLT组的患者在基线至六个月期间抑郁恶化也明显较少(p=0.006)。
护士主导的滴定门诊通过增加达到最大剂量的患者比例并促进慢性HFrEF患者快速上调β-肾上腺素能受体阻滞剂剂量,改善了β-肾上腺素能受体阻滞剂治疗的优化。
澳大利亚临床试验注册中心(ACTRN012606000383561)。