Jin Hong, Tang Chengchun, Wei Qin, Chen Long, Sun Qin, Ma Genshan, Liu Naifeng
Department of Cardiology, Zhongda Hospital, Medical School of Southeast University, 210009 Nanjing, Jiangsu, China.
BMC Cardiovasc Disord. 2014 Sep 24;14:127. doi: 10.1186/1471-2261-14-127.
Few studies have evaluated age-related predictors associated with the underuse of medications in patients with coronary heart disease (CHD). The objective of this study was to identify age-related differences in the factors associated with the underuse of recommended medications in patients diagnosed with acute coronary syndrome (ACS).
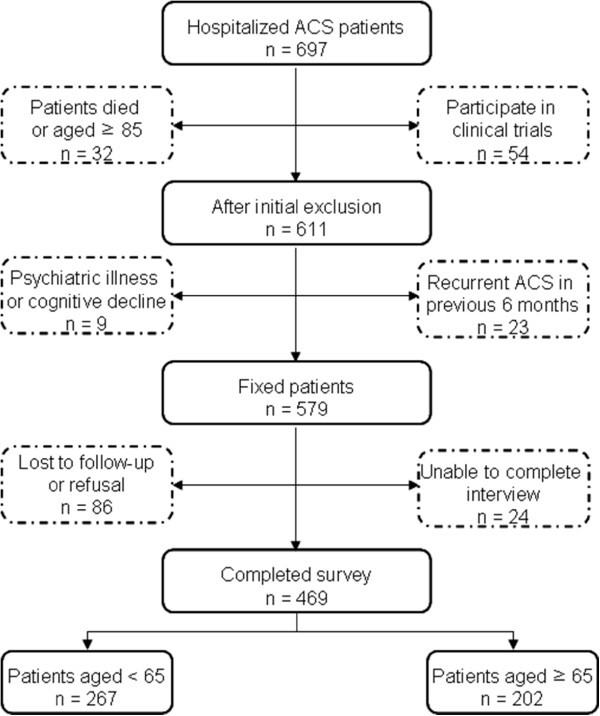
From August 2009 to April 2011, we recruited 469 consecutive ACS patients from a cardiac center at a university hospital. We divided the patients into older (65 years of age and older, n = 202) and younger groups (younger than 65 years of age, n = 267). Data on socio-demographic characteristics, depressive symptoms, and medication use were obtained from a telephone survey administered 18 to 24 months after hospital discharge. Additionally, we asked the patients to provide reasons for not taking their medications.
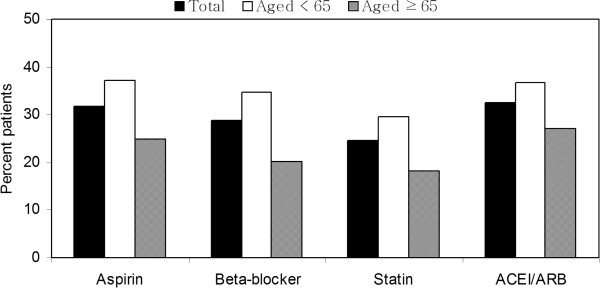
A significantly increased underuse of medication was noted in older patients compared with younger patients, including aspirin (24.8% vs. 37.1%, p = 0.005), beta-blockers (20.3% vs. 34.8%, p = 0.001), ACE inhibitor/angiotensin receptor blockers (27.2% vs. 36.7%, p = 0.030), and statins (21.8% vs. 29.6%, p = 0.005). Among older patients, the factors associated with the underuse of medications included low education level (odds ratio [OR], 3.93), greater number of comorbidities (OR, 1.64), and total number of discharge medications (OR, 1.31). The reasons provided by older patients for not taking medication included the fact that the medication was considered to be non-essential and the large number of medications. Among younger patients, low income (OR, 3.97) and depression (OR, 2.62) were predictors for underuse of medication, and the reasons provided for not taking medications included high costs and the fear of adverse effects.
At least one year after ACS hospital discharge, the underuse of recommended medications is related to low education level, comorbidities, and the total number of discharge medications in elderly patients, whereas underuse in younger patients is associated with low income and depression. The disparities related to these different predictors may have implications for age-related interventions targeting secondary preventions in CHD patients to improve their use of medication.
很少有研究评估与冠心病(CHD)患者药物使用不足相关的年龄相关预测因素。本研究的目的是确定在诊断为急性冠状动脉综合征(ACS)的患者中,与推荐药物使用不足相关的因素的年龄差异。
2009年8月至2011年4月,我们从一所大学医院的心脏中心连续招募了469例ACS患者。我们将患者分为老年组(65岁及以上,n = 202)和年轻组(65岁以下,n = 267)。社会人口学特征、抑郁症状和药物使用数据来自出院后18至24个月进行的电话调查。此外,我们询问患者不服用药物的原因。
与年轻患者相比,老年患者药物使用不足显著增加,包括阿司匹林(24.8%对37.1%,p = 0.005)、β受体阻滞剂(20.3%对34.8%,p = 0.001)、ACE抑制剂/血管紧张素受体阻滞剂(27.2%对36.7%,p = 0.030)和他汀类药物(21.8%对29.6%,p = 0.005)。在老年患者中,与药物使用不足相关的因素包括低教育水平(比值比[OR],3.93)、更多的合并症(OR,1.64)和出院药物总数(OR,1.31)。老年患者不服用药物的原因包括认为药物不必要和药物数量多。在年轻患者中,低收入(OR,3.97)和抑郁(OR,2.62)是药物使用不足的预测因素;不服用药物的原因包括费用高和担心不良反应。
ACS出院后至少一年,老年患者推荐药物使用不足与低教育水平、合并症和出院药物总数有关,而年轻患者使用不足与低收入和抑郁有关。这些不同预测因素相关的差异可能对针对CHD患者二级预防的年龄相关干预措施有影响,以改善他们的药物使用情况。