Hung Tsung-Hsing, Tseng Chih-Wei, Tseng Kuo-Chih, Hsieh Yu-Hsi, Tsai Chih-Chun, Tsai Chen-Chi
Division of Gastroenterology (T-HH, C-WT, K-CT, Y-HH), Department of Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi; School of Medicine (T-HH, C-WT, K-CT, Y-HH, C-Chi Tsai), Tzu Chi University, Hualien; Department of Mathematics (C-Chun Tsai), Tamkang University, Tamsui; Division of Infectious Disease (C-Chi Tsai), Department of Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan.
Medicine (Baltimore). 2014 Sep;93(14):e79. doi: 10.1097/MD.0000000000000079.
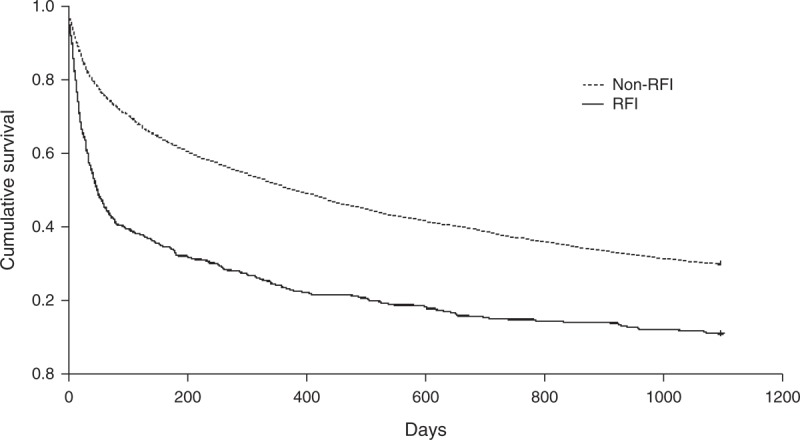
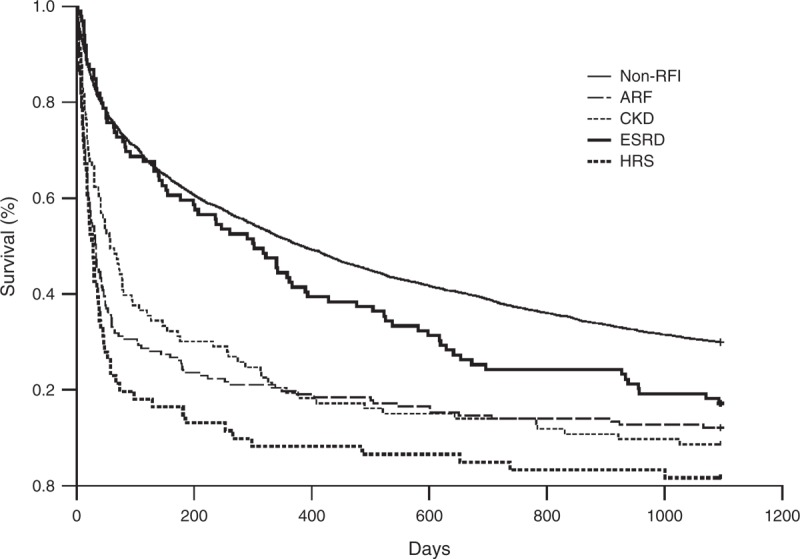
Kidney is an important organ to clear neurotoxic substance in circulation. However, it is still unknown about the effect of renal function impairment (RFI) on the mortality of cirrhotic patients with hepatic encephalopathy (HE). We used the Taiwan National Health Insurance Database to identify 4932 cirrhotic patients with HE, hospitalized between January 1, 2007 and December 31, 2007. The enrolled patients were followed up individually for 3 years to identify their 3-year mortalities. There were 411 (8.3%) patients with RFI and 4521 (91.7%) patients without RFI. The adjusted hazard ratio (HR) of RFI for 3-year mortality was 2.03 (95% CI, 1.82-2.27). In RFI group, there were 157 (38.2%) patients with acute renal failure (ARF), 61 (14.8%) with hepatorenal syndrome (HRS), 93 (22.6%) with chronic kidney disease (CKD), and 100 (24.3%) with end-stage renal disease (ESRD). Compared with the non-RFI group, the adjusted HR of ARF for 3-year mortality was 2.57 (95% CI, 2.17-3.06), CKD 1.93 (95% CI, 1.55-2.40), ESRD 1.26 (95% CI, 1.01-1.57), and HRS 3.58 (95% CI, 2.78-4.63). Among ESRD patients, there were 99 patients receiving hemodialysis regularly. Compared with the CKD group, the adjusted HR of ESRD with hemodialysis for 3-year mortality was 0.664 (95% CI, 0.466-0.945). RFI increased the 3-year mortality of cirrhotic patients with HE, especially ARF and HRS. HE patients with ESRD receiving hemodialysis had better 3-year survival rate than those with CKD.
肾脏是清除循环中神经毒性物质的重要器官。然而,肾功能损害(RFI)对肝硬化合并肝性脑病(HE)患者死亡率的影响仍不清楚。我们利用台湾全民健康保险数据库,确定了2007年1月1日至2007年12月31日期间住院的4932例肝硬化合并HE患者。对纳入的患者进行了3年的个体随访,以确定他们的3年死亡率。有411例(8.3%)患者存在RFI,4521例(91.7%)患者不存在RFI。RFI导致3年死亡率的调整后风险比(HR)为2.03(95%CI,1.82-2.27)。在RFI组中,有157例(38.2%)患者发生急性肾衰竭(ARF),61例(14.8%)患者发生肝肾综合征(HRS),93例(22.6%)患者患有慢性肾脏病(CKD),100例(24.3%)患者患有终末期肾病(ESRD)。与非RFI组相比,ARF导致3年死亡率的调整后HR为2.57(95%CI,2.17-3.06),CKD为1.93(95%CI,1.55-2.40),ESRD为1.26(95%CI,1.01-1.57),HRS为3.58(95%CI,2.78-4.63)。在ESRD患者中,有99例患者定期接受血液透析。与CKD组相比,接受血液透析的ESRD患者3年死亡率的调整后HR为0.664(95%CI,0.466-0.945)。RFI增加了肝硬化合并HE患者的3年死亡率,尤其是ARF和HRS。接受血液透析的ESRD的HE患者3年生存率高于CKD患者。