Jeong Jin Hee, Park In Sung, Kim Dong Hoon, Kim Seong Chun, Kang Changwoo, Lee Soo Hoon, Kim Tae Yun, Lee Sang Bong
aDepartment of Emergency Medicine, Gyeongsang National University School of Medicine, Jinju-si, Gyeongsangnam-do, Republic of Korea bDepartment of Neurosurgery, Gyeongsang National University School of Medicine, Jinju-si, Gyeongsangnam-do, Republic of Korea cGyeongsang Institute of Health Sciences, Gyeongsang National University School of Medicine, Jinju-si, Gyeongsangnam-do, Republic of Korea.
Medicine (Baltimore). 2016 Jun;95(26):e3935. doi: 10.1097/MD.0000000000003935.
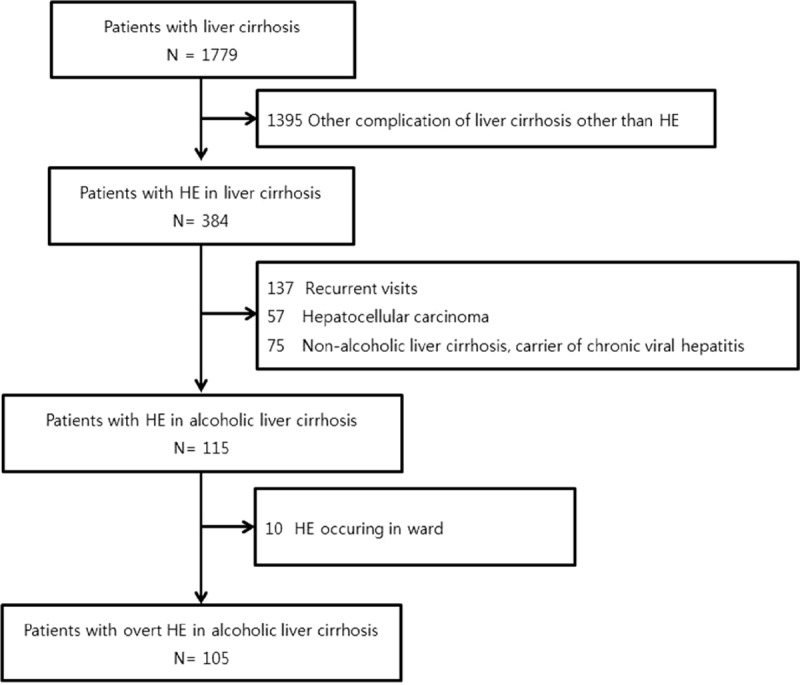
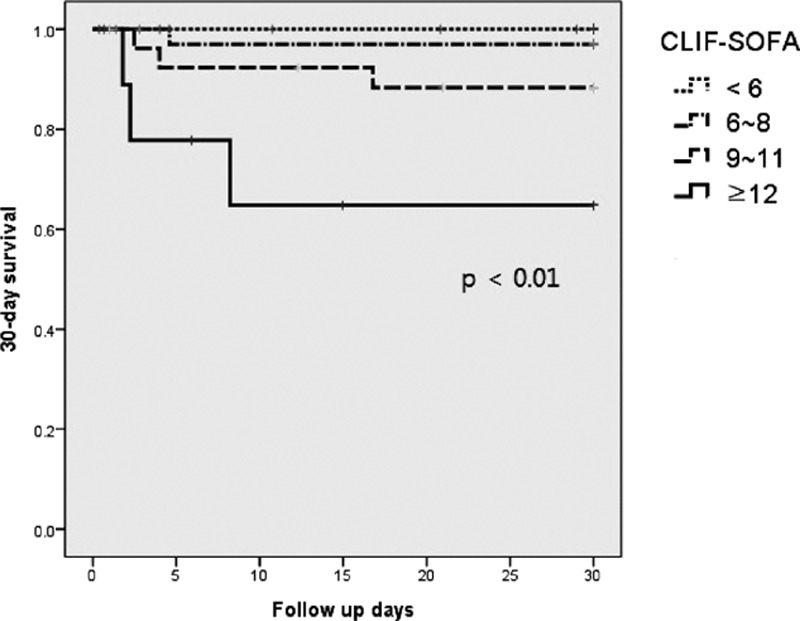
Hepatic encephalopathy (HE) is a complication associated with worst prognosis in decompensated liver cirrhosis (LC) patients. Previous studies have identified prognostic factors for HE, and recent studies reported an association between systemic inflammatory response syndrome (SIRS) and liver disease. This study aimed to identify prognostic factors for 30-day mortality in alcoholic LC patients with HE who visited the emergency department (ED).This was a retrospective study of alcoholic LC patients with HE from January 1, 2010, to April 30, 2015. The baseline characteristics, complications of portal hypertension, laboratory values, Child-Pugh class, Model for End-stage Liver Disease (MELD) score, chronic liver failure-sequential organ failure assessment (CLIF-SOFA) score, and SIRS criteria were assessed. The presence of 2 or more SIRS criteria was considered SIRS. The primary outcomes were 30-day mortality and prognostic factors for patients with HE visiting the ED.In total, 105 patients who met the inclusion criteria were analyzed. Overall, the 30-day mortality rate was 6.7% (7 patients).Significant variables were hepatorenal syndrome, international normalized ratio, white blood cell count, total bilirubin level, MELD score CLIF-SOFA score, and SIRS in univariate analysis. CLIF-SOFA score and SIRS were the significant factors in the multivariate analysis (hazard ratio 5.56, 15.98; 95% confidence interval 1.18-26.18, 1.58-161.37; P = 0.03, P = 0.02). The mortality rates differed according to the CLIF-SOFA score (P < 0.01).The CLIF-SOFA score and SIRS in alcoholic LC patients with HE visiting the ED are independent predictors of 30-day mortality.
肝性脑病(HE)是失代偿期肝硬化(LC)患者预后最差的一种并发症。既往研究已确定了HE的预后因素,近期研究报道了全身炎症反应综合征(SIRS)与肝脏疾病之间的关联。本研究旨在确定就诊于急诊科(ED)的酒精性LC合并HE患者30天死亡率的预后因素。
这是一项对2010年1月1日至2015年4月30日期间酒精性LC合并HE患者的回顾性研究。评估了基线特征、门静脉高压并发症、实验室检查值、Child-Pugh分级、终末期肝病模型(MELD)评分、慢性肝衰竭-序贯器官衰竭评估(CLIF-SOFA)评分以及SIRS标准。存在2项或更多SIRS标准被视为SIRS。主要结局是就诊于ED的HE患者的30天死亡率及预后因素。
总共分析了105例符合纳入标准的患者。总体而言,30天死亡率为6.7%(7例患者)。
单因素分析中,显著变量为肝肾综合征、国际标准化比值、白细胞计数、总胆红素水平、MELD评分、CLIF-SOFA评分和SIRS。多因素分析中,CLIF-SOFA评分和SIRS是显著因素(风险比5.56,15.98;95%置信区间1.18 - 26.18,1.58 - 161.37;P = 0.03,P = 0.02)。死亡率根据CLIF-SOFA评分不同而有所差异(P<0.01)。
就诊于ED的酒精性LC合并HE患者的CLIF-SOFA评分和SIRS是30天死亡率的独立预测因素。