Demirgan Serdar, Erkalp Kerem, Sevdi M Salih, Aydogmus Meltem Turkay, Kutbay Numan, Firincioglu Aydin, Ozalp Ali, Alagol Aysin
Department of Anesthesiology and Reanimation, Bagcilar Educational and Training Hospital, Şenlikköy Mah, İncir Sokak, No:1/3, Sarı Konaklar Sitesi, B-Blok, Daire:6, Florya/ Bakırköy, Istanbul, Turkey.
BMC Anesthesiol. 2014 Sep 18;14:78. doi: 10.1186/1471-2253-14-78. eCollection 2014.
Hypothermia has been used in cardiac surgery for many years for neuroprotection. Mild hypothermia (MH) [body temperature (BT) kept at 32-35°C] has been shown to reduce both mortality and poor neurological outcome in patients after cardiopulmonary resuscitation (CPR). This study investigated whether patients who were expected to benefit neurologically from therapeutic hypothermia (TH) also had improved cardiac function.
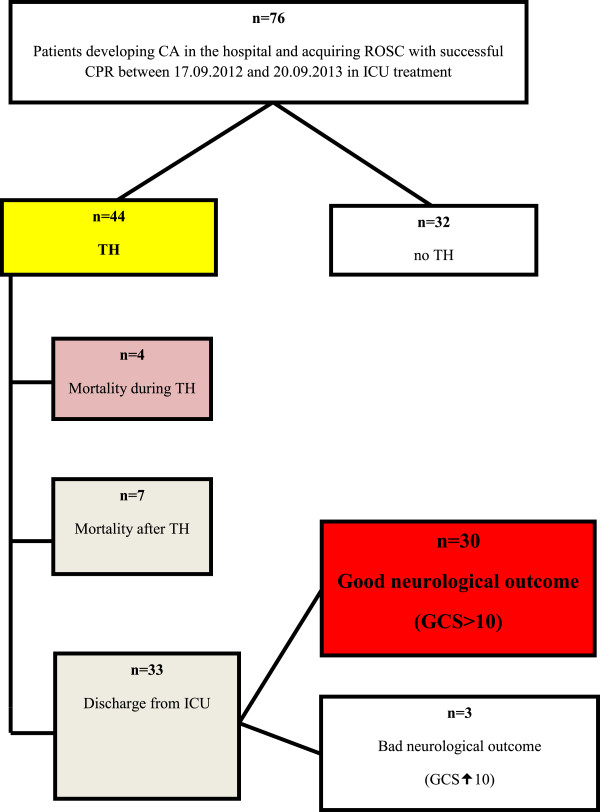
The study included 30 patients who developed in-hospital cardiac arrest between September 17, 2012, and September 20, 2013, and had return of spontaneous circulation (ROSC) following successful CPR. Patient BTs were cooled to 33°C using intravascular heat change. Basal BT, systolic artery pressure (SAP), diastolic artery pressure (DAP), mean arterial pressure (MAP), heart rate, central venous pressure, cardiac output (CO), cardiac index (CI), global end-diastolic volume index (GEDI), extravascular lung water index (ELWI), and systemic vascular resistance index (SVRI) were measured at 36°C, 35°C, 34°C and 33°C during cooling. BT was held at 33°C for 24 hours prior to rewarming. Rewarming was conducted 0.25°C/h. During rewarming, measurements were repeated at 33°C, 34°C, 35°C and 36°C. A final measurement was performed once patients spontaneously returned to basal BT. We compared cooling and rewarming cardiac measurements at the same BTs.
SAP values during rewarming (34°C, 35°C and 36°C) were lower than during cooling (P < 0.05). DAP values during rewarming (basal temperature, 34°C, 35°C and 36°C) were lower than during cooling. MAP values during rewarming (34°C, 35°C and 36°C) were lower than during cooling (P < 0.05). CO and CI values were higher during rewarming than during cooling. GEDI and ELWI did not differ during cooling and rewarming. SVRI values during rewarming (34°C, 35°C, 36°C and basal temperature) were lower than during cooling (P < 0.05).
To our knowledge, this is the first study comparing cardiac function at the same BTs during cooling and rewarming. In patients experiencing ROSC following CPR, TH may improve cardiac function and promote favorable neurological outcomes.
低温技术在心脏手术中用于神经保护已有多年。轻度低温(MH)[体温(BT)维持在32 - 35°C]已被证明可降低心肺复苏(CPR)后患者的死亡率和不良神经结局。本研究调查了预期从治疗性低温(TH)中获得神经益处的患者其心脏功能是否也得到改善。
该研究纳入了2012年9月17日至2013年9月20日期间在医院发生心脏骤停且成功进行CPR后恢复自主循环(ROSC)的30例患者。使用血管内热交换将患者体温降至33°C。在降温过程中,于36°C、35°C、34°C和33°C时测量基础体温、收缩压(SAP)、舒张压(DAP)、平均动脉压(MAP)、心率、中心静脉压、心输出量(CO)、心脏指数(CI)、全心舒张末期容积指数(GEDI)、血管外肺水指数(ELWI)和全身血管阻力指数(SVRI)。在复温前将体温维持在33°C 24小时。以0.25°C/小时的速度进行复温。在复温过程中,于33°C、34°C、35°C和36°C时重复测量。一旦患者自发恢复到基础体温,进行最后一次测量。我们比较了相同体温下降温及复温过程中的心脏测量值。
复温期间(34°C、35°C和36°C)的SAP值低于降温期间(P < 0.05)。复温期间(基础体温、34°C、35°C和36°C)的DAP值低于降温期间。复温期间(34°C、35°C和36°C)的MAP值低于降温期间(P < 0.05)。复温期间的CO和CI值高于降温期间。GEDI和ELWI在降温和复温期间无差异。复温期间(34°C、35°C、36°C和基础体温)的SVRI值低于降温期间(P < 0.05)。
据我们所知,这是第一项比较降温和复温过程中相同体温下心脏功能的研究。在CPR后恢复自主循环的患者中,TH可能改善心脏功能并促进良好的神经结局。