Pezawas Thomas, Diedrich André, Winker Robert, Robertson David, Richter Bernhard, Wang Li, Byrne Daniel W, Schmidinger Herwig
From the Division of Cardiology, Department of Internal Medicine II, Medical University of Vienna, Vienna, Austria (T.P., B.R., H.S.); Departments of Medicine (A.D.), and Departments of Medicine, Pharmacology, Neurology (D.R.), Division of Clinical Pharmacology, Vanderbilt Autonomic Dysfunction Center, Vanderbilt University School of Medicine, Nashville, TN; Health and Prevention Center, Sanatorium Hera, Vienna, Austria (R.W.); and Department of Biostatistics, Vanderbilt University School of Medicine, Nashville, TN (L.W., D.W.B.).
Circ Arrhythm Electrophysiol. 2014 Dec;7(6):1101-8. doi: 10.1161/CIRCEP.114.001745. Epub 2014 Sep 27.
Prophylactic defibrillator implantation is recommended in dilated, nonischemic heart disease and left ventricular ejection fraction of ≤0.30 to 0.35. Noninvasive testing should improve accuracy in decision making of prophylactic defibrillator implantation.
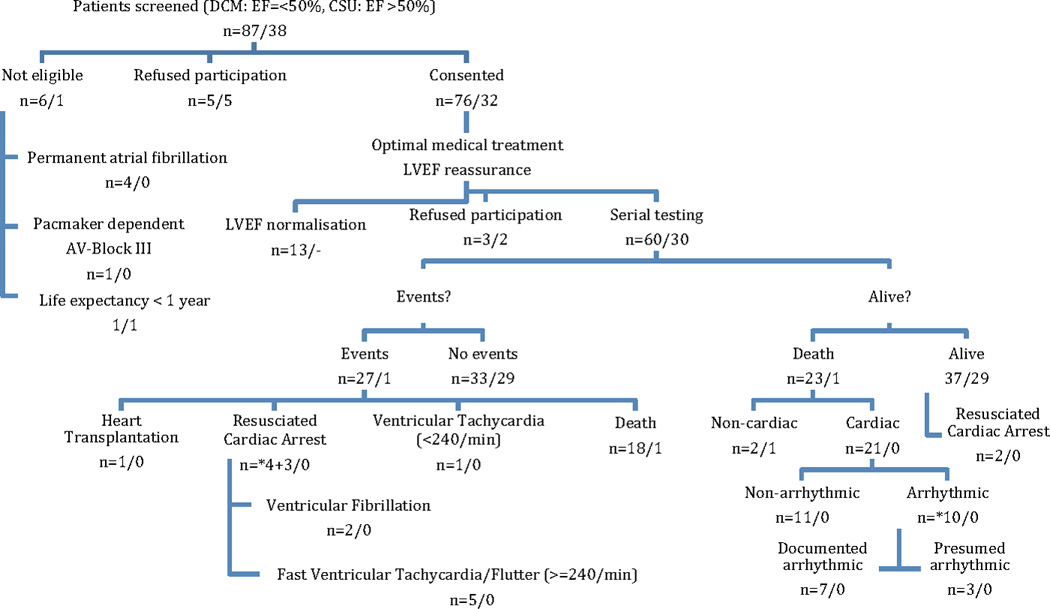
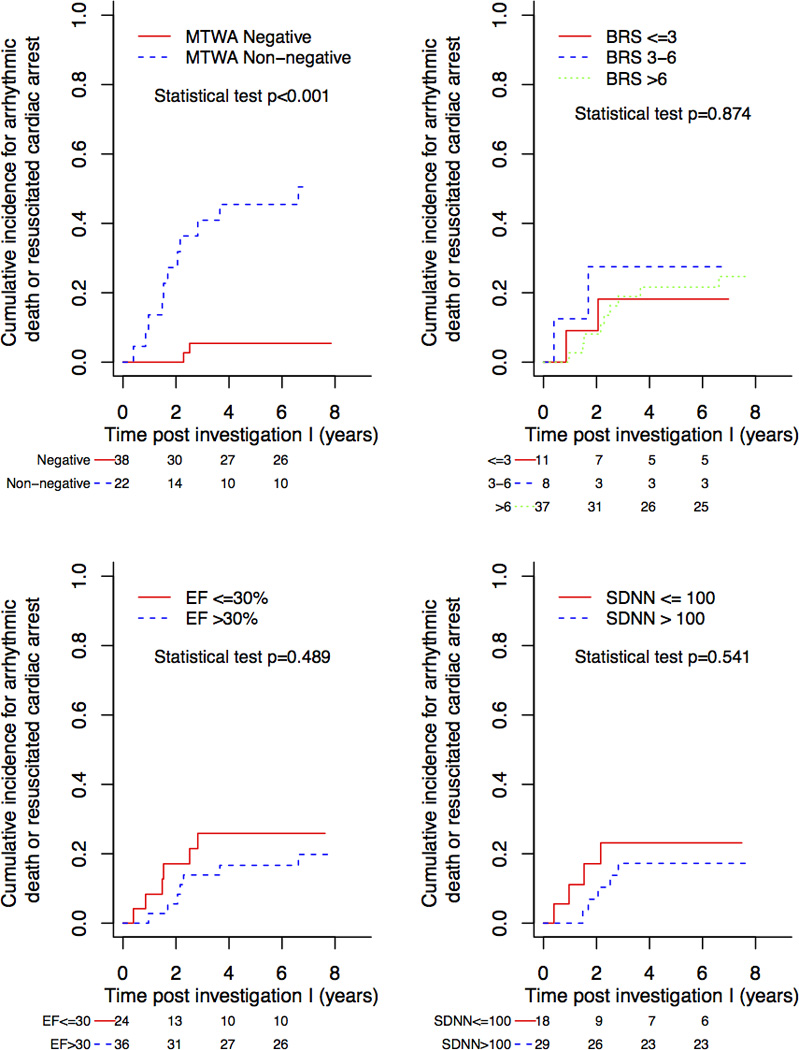
We enrolled 60 patients (median age, 57 years) with dilated cardiomyopathy and left ventricular ejection fraction ≤0.50, and 30 control subjects (median age, 59 years) with left ventricular ejection fraction >0.50. The protocol included an initial assessment, a second assessment after 3 years, and a final follow-up: pharmacological baroreflex testing (baroreceptor reflex sensitivity), short-term spectral analysis of heart rate variability (low frequency/high frequency), and long-term time domain analysis (SD of all normal-to-normal R-R intervals), exercise microvolt T wave alternans, and signal-averaged ECG, and corrected QT-time. The median follow-up was 7 years. End points were cardiac death, resuscitated cardiac arrest, and arrhythmic death. Cardiac death was observed in 21 patients. Resuscitated cardiac arrest and arrhythmic death caused by ventricular tachyarrhythmias ≥240 per minute was observed in 7 and 10 patients, respectively. In the single time point analysis, microvolt T wave alternans, baroreceptor reflex sensitivity, and SD of all normal-to-normal R-R intervals at initial testing added significant information regarding cardiac death. Microvolt T wave alternans added information on resuscitated cardiac arrest or arrhythmic death at multiple time points (P<0.001). False-negative microvolt T wave alternans results were seen in 8% of patients.
Noninvasive testing and left ventricular ejection fraction could not reliably identify patients with dilated cardiomyopathy at risk of fatal ventricular tachyarrhythmias. Therefore, the strategy to confine prophylactic implantable cardioverter-defibrillator implantation to patients with dilated cardiomyopathy and severely reduced LV function should be reconsidered.
对于扩张型非缺血性心脏病且左心室射血分数≤0.30至0.35的患者,推荐植入预防性除颤器。非侵入性检测应能提高预防性除颤器植入决策的准确性。
我们纳入了60例扩张型心肌病且左心室射血分数≤0.50的患者(中位年龄57岁)以及30例左心室射血分数>0.50的对照受试者(中位年龄59岁)。研究方案包括初始评估、3年后的第二次评估以及最终随访:药物压力反射测试(压力感受器反射敏感性)、心率变异性的短期频谱分析(低频/高频)、长期时域分析(所有正常R-R间期的标准差)、运动微伏T波交替变化、信号平均心电图以及校正QT间期。中位随访时间为7年。终点为心源性死亡、复苏的心脏骤停以及心律失常性死亡。21例患者发生心源性死亡。分别有7例和10例患者发生了每分钟≥240次室性快速心律失常所致的复苏心脏骤停和心律失常性死亡。在单时间点分析中,初始检测时的微伏T波交替变化、压力感受器反射敏感性以及所有正常R-R间期的标准差为心源性死亡提供了重要信息。微伏T波交替变化在多个时间点为复苏心脏骤停或心律失常性死亡提供了信息(P<0.001)。8%的患者出现微伏T波交替变化假阴性结果。
非侵入性检测和左心室射血分数无法可靠地识别扩张型心肌病有致命性室性快速心律失常风险的患者。因此,应重新考虑将预防性植入式心律转复除颤器植入仅限于扩张型心肌病且左心室功能严重降低患者的策略。