Centro de Estudos de Doenças Crónicas, CEDOC, NOVA Medical School/Faculdade de Ciências Médicas, Universidade Nova de Lisboa Lisboa, Portugal.
Front Physiol. 2014 Sep 22;5:361. doi: 10.3389/fphys.2014.00361. eCollection 2014.
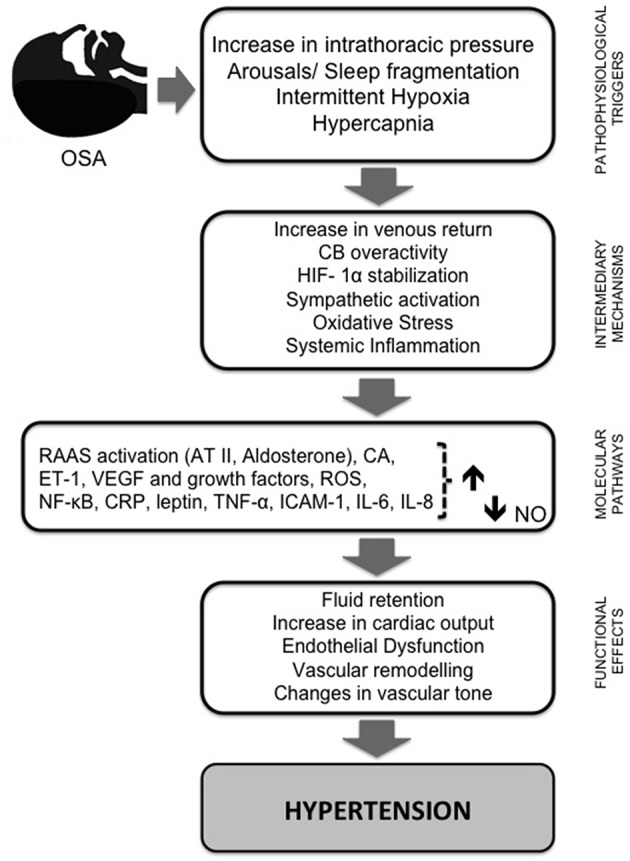
Sleep apnea/hypopnea disorders include centrally originated diseases and obstructive sleep apnea (OSA). This last condition is renowned as a frequent secondary cause of hypertension (HT). The mechanisms involved in the pathogenesis of HT can be summarized in relation to two main pathways: sympathetic nervous system stimulation mediated mainly by activation of carotid body (CB) chemoreflexes and/or asphyxia, and, by no means the least important, the systemic effects of chronic intermittent hypoxia (CIH). The use of animal models has revealed that CIH is the critical stimulus underlying sympathetic activity and hypertension, and that this effect requires the presence of functional arterial chemoreceptors, which are hyperactive in CIH. These models of CIH mimic the HT observed in humans and allow the study of CIH independently without the mechanical obstruction component. The effect of continuous positive airway pressure (CPAP), the gold standard treatment for OSA patients, to reduce blood pressure seems to be modest and concomitant antihypertensive therapy is still required. We focus this review on the efficacy of pharmacological interventions to revert HT associated with CIH conditions in both animal models and humans. First, we explore the experimental animal models, developed to mimic HT related to CIH, which have been used to investigate the effect of antihypertensive drugs (AHDs). Second, we review what is known about drug efficacy to reverse HT induced by CIH in animals. Moreover, findings in humans with OSA are cited to demonstrate the lack of strong evidence for the establishment of a first-line antihypertensive regimen for these patients. Indeed, specific therapeutic guidelines for the pharmacological treatment of HT in these patients are still lacking. Finally, we discuss the future perspectives concerning the non-pharmacological and pharmacological management of this particular type of HT.
睡眠呼吸暂停/低通气障碍包括中枢性疾病和阻塞性睡眠呼吸暂停(OSA)。最后一种情况是众所周知的高血压(HT)的常见继发性原因。HT 发病机制中涉及的机制可以概括为两个主要途径:主要通过颈动脉体(CB)化学感受器激活介导的交感神经系统刺激和/或窒息,以及绝不是最不重要的,慢性间歇性低氧(CIH)的全身影响。动物模型的使用表明,CIH 是交感活性和高血压的关键刺激因素,并且这种效应需要功能性动脉化学感受器的存在,在 CIH 中化学感受器过度活跃。这些 CIH 模型模拟了在人类中观察到的 HT,并允许在没有机械阻塞成分的情况下独立研究 CIH。持续气道正压通气(CPAP)作为 OSA 患者的黄金标准治疗,降低血压的效果似乎温和,仍然需要同时进行降压治疗。我们将重点放在药物干预对逆转与 CIH 相关的 HT 的疗效上,无论是在动物模型还是在人类中。首先,我们探讨了模拟与 CIH 相关的 HT 的实验动物模型,这些模型用于研究降压药物(AHD)的作用。其次,我们回顾了已知的药物在逆转 CIH 引起的 HT 方面在动物中的疗效。此外,还引用了患有 OSA 的人类的发现,以证明缺乏为这些患者建立一线降压方案的有力证据。实际上,这些患者 HT 的药物治疗具体治疗指南仍然缺乏。最后,我们讨论了针对这种特殊类型 HT 的非药物和药物管理的未来前景。