Jolley Sarah E, Regan-Baggs Janet, Dickson Robert P, Hough Catherine L
Division of Pulmonary and Critical Care Medicine, University of Washington, Seattle, WA USA ; Division of Pulmonary and Critical Care Medicine, Harborview Medical Center, University of Washington, Campus Box 356522, Seattle, WA 98195-6522 USA.
Department of Nursing, University of Washington, Seattle, WA USA.
BMC Anesthesiol. 2014 Oct 1;14:84. doi: 10.1186/1471-2253-14-84. eCollection 2014.
Early mobilization (EM) of patients on mechanical ventilation (MV) is shown to improve outcomes after critical illness. Little is known regarding clinician knowledge of EM or multi-disciplinary barriers to use of EM in the intensive care unit (ICU). The goal of this study was to assess clinician knowledge regarding EM and identify barriers to its provision.
Simultaneous cross-sectional surveys of medical ICU (MICU) nurses (RN)/physical therapists (PT) respondents and physician (MD) respondents in a single MICU at an academic hospital in Seattle, WA in 2010-2011. Responses were indicated on a 5 point Likert scale and reported as proportion of respondents agreeing or disagreeing. Chi-square testing and Fisher's exact testing was performed to determine whether responses differed by duration of employment or prior EM experience.
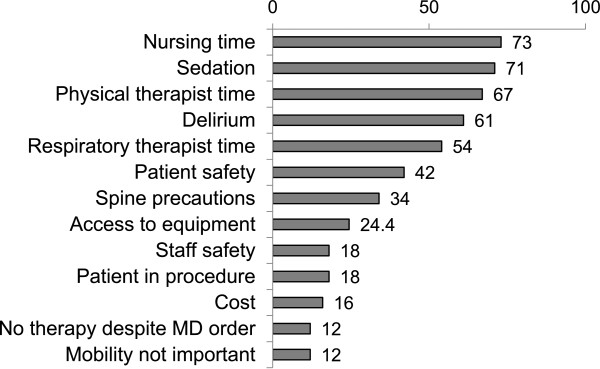
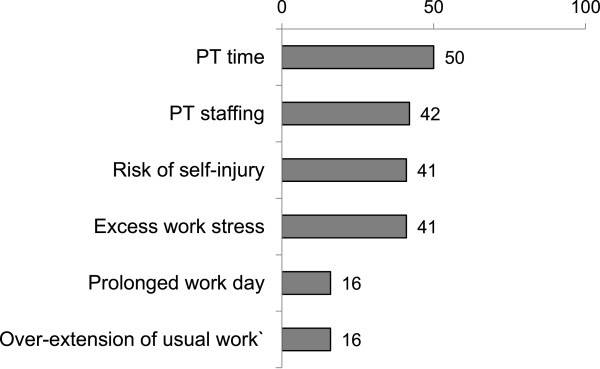
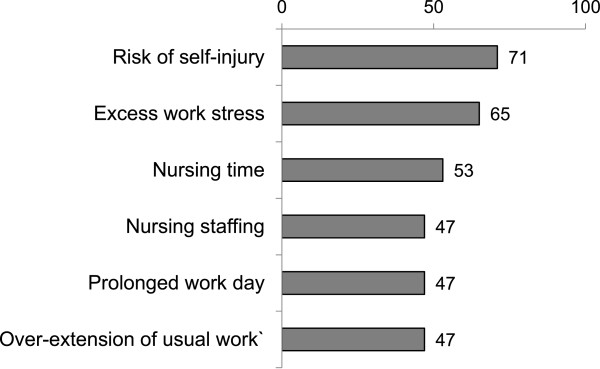
A total of 120 clinicians responded to the survey (91 MDs (response rate 82% (91/111)), 17 RNs (response rate 22%, (17/78)), and 12 PTs (response rate 86%, (12/14)), overall response rate 86%). Most clinicians indicated knowledge regarding benefits of EM. More attending physicians reported knowledge of EM benefits, but also that risks of EM outweigh the benefits compared to trainees (p = 0.02 and 0.01). Clinicians across disciplines reported near universal agreement to use of EM for patients on MV, while the minority reported agreement to EM for patients on vasoactive agents. The most frequently reported cross-disciplinary barriers to EM were staffing and time. Risk of self-injury and excess work stress were indicated as barriers by RN and PT respondents.
MICU clinicians, at our institution, reported knowledge of EM in the ICU. Staffing and clinician time were frequently identified cross-disciplinary barriers. Risk of self-injury and excess work stress were frequently reported RN and PT barriers.
机械通气(MV)患者的早期活动(EM)已被证明可改善危重症后的预后。对于重症监护病房(ICU)中临床医生对EM的了解或使用EM的多学科障碍知之甚少。本研究的目的是评估临床医生对EM的了解,并确定提供EM的障碍。
2010 - 2011年在华盛顿州西雅图一家学术医院的单个医学重症监护病房(MICU)对护士(RN)/物理治疗师(PT)受访者和医生(MD)受访者进行同步横断面调查。回答采用5点李克特量表表示,并报告为同意或不同意的受访者比例。进行卡方检验和费舍尔精确检验以确定回答是否因工作年限或先前的EM经验而有所不同。
共有120名临床医生回复了调查(91名医生(回复率82%(91/111)),17名护士(回复率22%,(17/78)),以及12名物理治疗师(回复率86%,(12/14)),总体回复率86%)。大多数临床医生表示了解EM的益处。更多的主治医生报告了解EM的益处,但也表示与实习生相比,EM的风险超过益处(p = 0.02和0.01)。各学科的临床医生报告几乎普遍同意对MV患者使用EM,而少数人报告同意对使用血管活性药物的患者进行EM。最常报告的EM跨学科障碍是人员配备和时间。护士和物理治疗师受访者指出自我伤害风险和过度工作压力是障碍。
在我们机构,MICU临床医生报告了对ICU中EM的了解。人员配备和临床医生时间是经常被确定的跨学科障碍。自我伤害风险和过度工作压力是护士和物理治疗师经常报告的障碍。