Ahn Shin-Young, Kim Sejoong, Kim Dong Ki, Park Jung Hwan, Shin Sung Joon, Lee Sang Ho, Choi Bum Soon, Lim Chun Soo, Kim Suhnggwon, Chin Ho Jun
Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. ; Department of Immunology, Seoul National University Postgraduate School, Seoul, Korea.
Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
J Korean Med Sci. 2014 Sep;29 Suppl 2(Suppl 2):S123-30. doi: 10.3346/jkms.2014.29.S2.S123. Epub 2014 Sep 30.
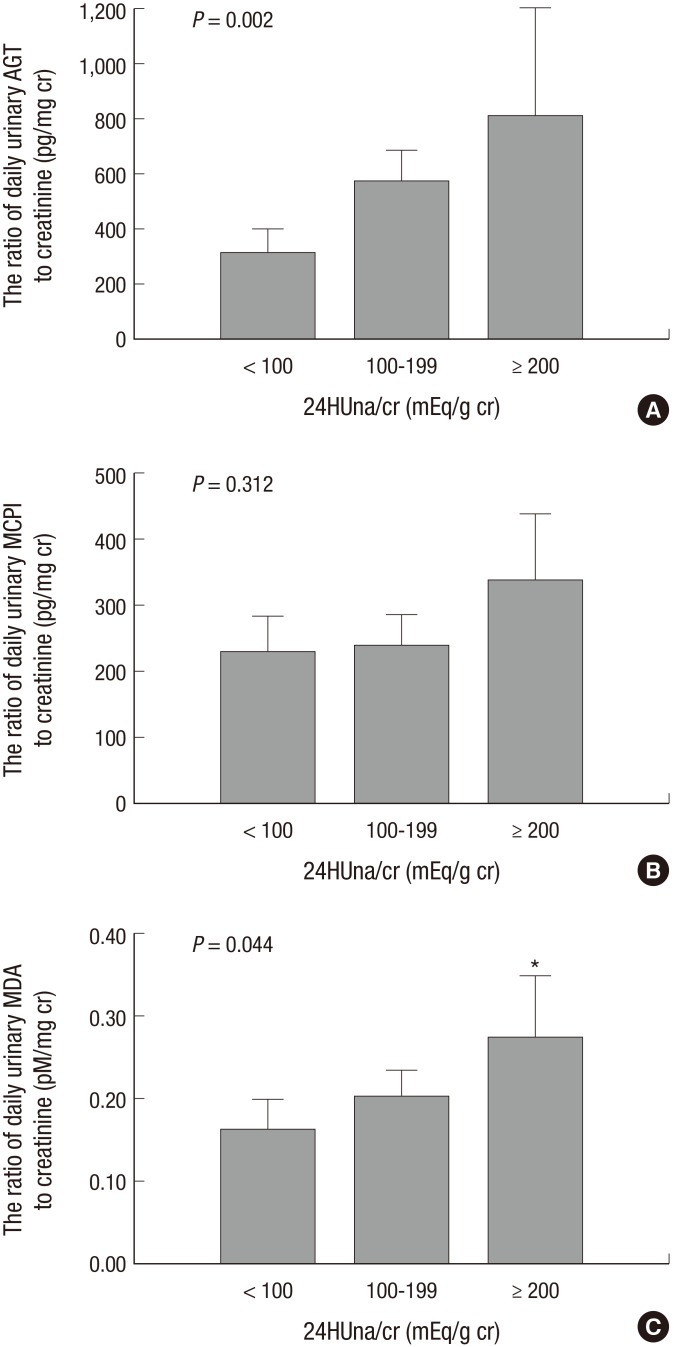
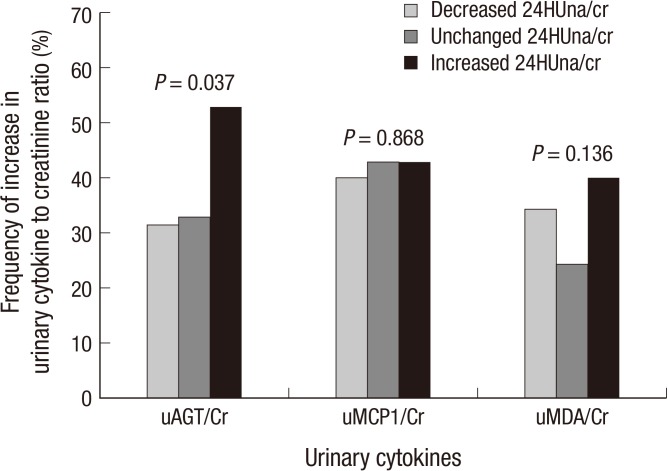
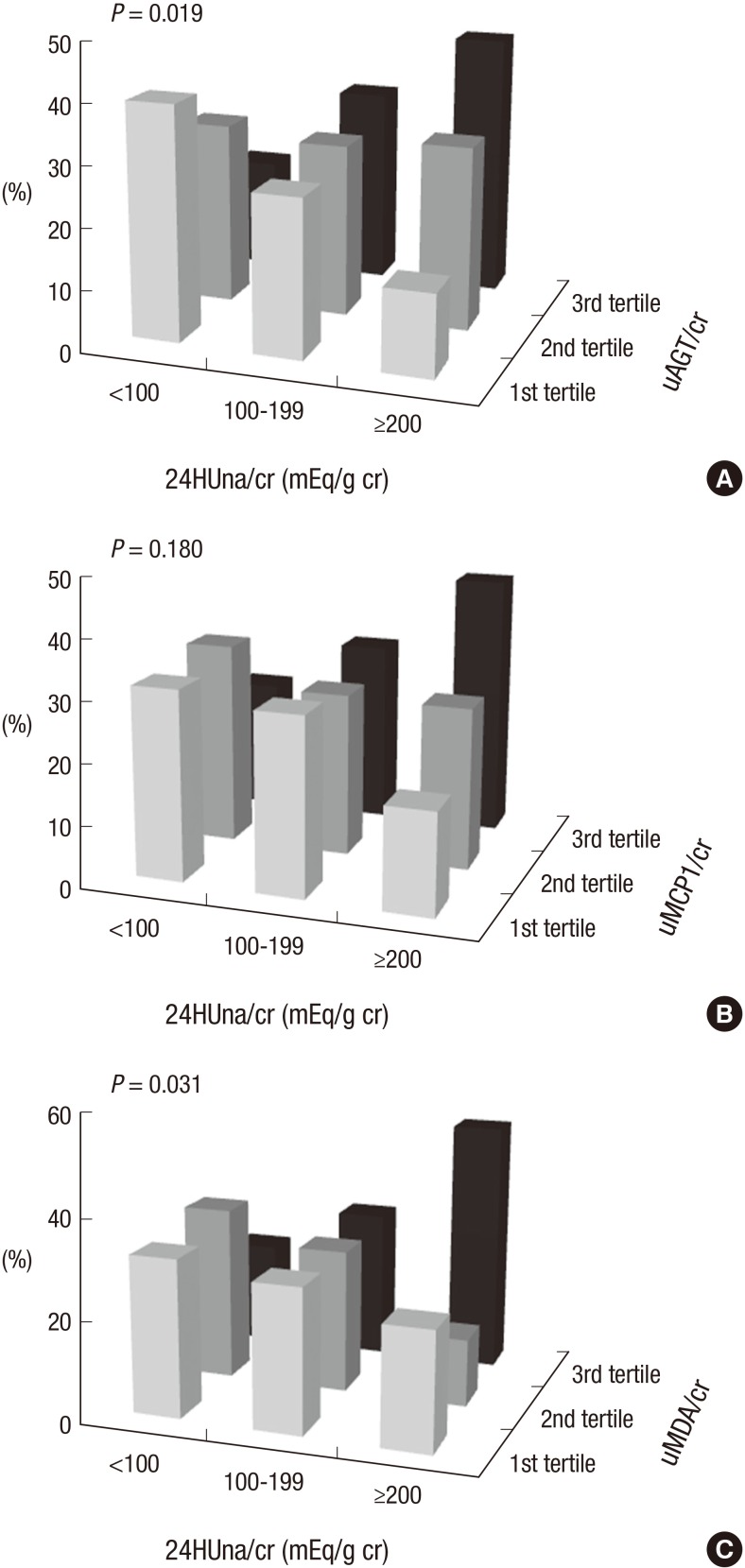
It is not well described the pathophysiology of renal injuries caused by a high salt intake in humans. The authors analyzed the relationship between the 24-hr urine sodium-to-creatinine ratio (24HUna/cr) and renal injury parameters such as urine angiotensinogen (uAGT/cr), monocyte chemoattractant peptide-1 (uMCP1/cr), and malondialdehyde-to-creatinine ratio (uMDA/cr) by using the data derived from 226 hypertensive chronic kidney disease patients. At baseline, the 24HUna/cr group or levels had a positive correlation with uAGT/cr and uMDA/cr adjusted for related factors (P<0.001 for each analysis). When we estimated uAGT/cr in the 24HUna/cr groups by ANCOVA, the uAGT/cr in patients with ≥200 mEq/g cr was higher than in patients with <100 mEq/g cr (708 [95% CI, 448-967] vs. 334 [95% CI, 184-483] pg/mg cr, P=0.014). Similarly, uMDA/cr was estimated as 0.17 (95% CI, 0.14-0.21) pM/mg cr in patients with <100 mEq/g cr and 0.27 (95% CI, 0.20-0.33) pM/mg cr in patients with ≥200 mEq/g cr (P=0.016). During the 16-week follow-up period, an increase in urinary sodium excretion predicted an increase in urinary angiotensinogen excretion. In conclusion, high salt intake increases renal renin-angiotensin-system (RAS) activation, primarily, and directly or indirectly affects the production of reactive oxygen species through renal RAS activation.
高盐摄入导致人类肾损伤的病理生理学尚未得到充分描述。作者利用226例高血压慢性肾病患者的数据,分析了24小时尿钠肌酐比值(24HUna/cr)与肾损伤参数之间的关系,这些参数包括尿血管紧张素原(uAGT/cr)、单核细胞趋化蛋白-1(uMCP1/cr)以及丙二醛肌酐比值(uMDA/cr)。在基线时,校正相关因素后,24HUna/cr组或水平与uAGT/cr和uMDA/cr呈正相关(每项分析P<0.001)。当我们通过协方差分析估计24HUna/cr组中的uAGT/cr时,24HUna/cr≥200 mEq/g cr的患者的uAGT/cr高于<100 mEq/g cr的患者(708 [95% CI,448 - 967] vs. 334 [95% CI,184 - 483] pg/mg cr,P = 0.014)。同样,<100 mEq/g cr的患者的uMDA/cr估计为0.17(95% CI,0.14 - 0.21)pM/mg cr,而≥200 mEq/g cr的患者为0.27(95% CI,0.20 - 0.33)pM/mg cr(P = 0.016)。在16周的随访期内,尿钠排泄增加预示着尿血管紧张素原排泄增加。总之,高盐摄入主要增加肾素-血管紧张素系统(RAS)的激活,并通过肾RAS激活直接或间接影响活性氧的产生。