Lopes de Campos Walter R, Chirwa Nthato, London Grace, Rotherham Lia S, Morris Lynn, Mayosi Bongani M, Khati Makobetsa
Emerging Health Technologies Competency Area, Biosciences Unit, Council for Scientific and Industrial Research, Pretoria, South Africa.
National Institute for Communicable Diseases, Sandringham, South Africa.
PLoS One. 2014 Oct 17;9(10):e110930. doi: 10.1371/journal.pone.0110930. eCollection 2014.
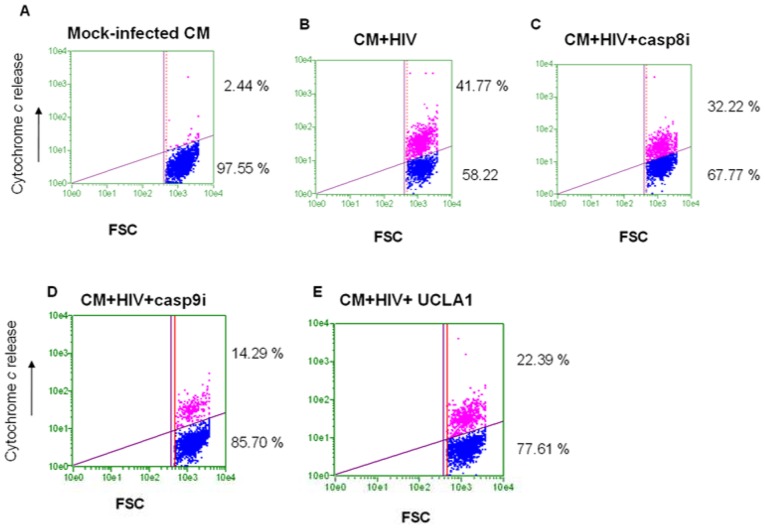
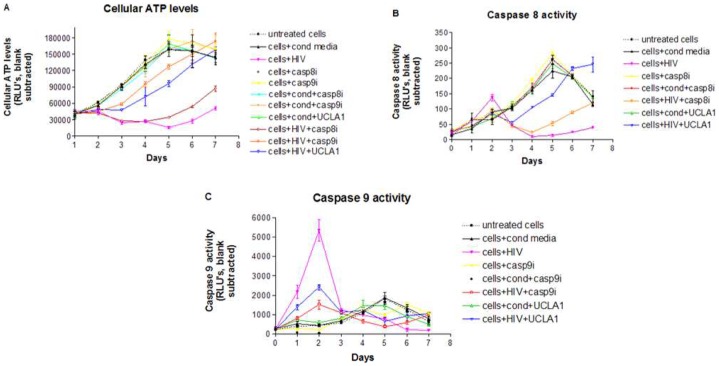
HIV-associated cardiomyopathy (HIVCM) is of clinical concern in developing countries because of a high HIV-1 prevalence, especially subtype C, and limited access to highly active antiretroviral therapy (HAART). For these reasons, we investigated the direct and indirect effects of HIV-1 subtype C infection of cultured human cardiomyocytes and the mechanisms leading to cardiomyocytes damage; as well as a way to mitigate the damage. We evaluated a novel approach to mitigate HIVCM using a previously reported gp120 binding and HIV-1 neutralizing aptamer called UCLA1. We established a cell-based model of HIVCM by infecting human cardiomyocytes with cell-free HIV-1 or co-culturing human cardiomyocytes with HIV-infected monocyte derived macrophages (MDM). We discovered that HIV-1 subtype C unproductively (i.e. its life cycle is arrested after reverse transcription) infects cardiomyocytes. Furthermore, we found that HIV-1 initiates apoptosis of cardiomyocytes through caspase-9 activation, preferentially via the intrinsic or mitochondrial initiated pathway. CXCR4 receptor-using viruses were stronger inducers of apoptosis than CCR5 utilizing variants. Importantly, we discovered that HIV-1 induced apoptosis of cardiomyocytes was mitigated by UCLA1. However, UCLA1 had no protective effective on cardiomyocytes when apoptosis was triggered by HIV-infected MDM. When HIV-1 was treated with UCLA1 prior to infection of MDM, it failed to induce apoptosis of cardiomyocytes. These data suggest that HIV-1 causes a mitochondrial initiated apoptotic cascade, which signal through caspase-9, whereas HIV-1 infected MDM causes apoptosis predominantly via the death-receptor pathway, mediated by caspase-8. Furthermore the data suggest that UCLA1 protects cardiomyocytes from caspase-mediated apoptosis, directly by binding to HIV-1 and indirectly by preventing infection of MDM.
由于人类免疫缺陷病毒1型(HIV-1),尤其是C亚型的高流行率以及获得高效抗逆转录病毒疗法(HAART)的机会有限,HIV相关心肌病(HIVCM)在发展中国家成为临床关注的问题。基于这些原因,我们研究了HIV-1 C亚型感染培养的人类心肌细胞的直接和间接影响以及导致心肌细胞损伤的机制;还有减轻这种损伤的方法。我们评估了一种使用先前报道的名为UCLA1的gp120结合和HIV-1中和适体来减轻HIVCM的新方法。我们通过用无细胞HIV-1感染人类心肌细胞或将人类心肌细胞与HIV感染的单核细胞衍生巨噬细胞(MDM)共培养,建立了HIVCM的细胞模型。我们发现HIV-1 C亚型非生产性地(即其生命周期在逆转录后停滞)感染心肌细胞。此外,我们发现HIV-1通过激活半胱天冬酶-9引发心肌细胞凋亡,优先通过内源性或线粒体启动途径。使用CXCR4受体的病毒比使用CCR5的变体更能诱导凋亡。重要的是,我们发现UCLA1减轻了HIV-1诱导的心肌细胞凋亡。然而,当由HIV感染的MDM触发凋亡时,UCLA1对心肌细胞没有保护作用。当在MDM感染之前用UCLA1处理HIV-1时,它未能诱导心肌细胞凋亡。这些数据表明,HIV-1导致线粒体启动的凋亡级联反应,通过半胱天冬酶-9发出信号,而HIV-1感染的MDM主要通过由半胱天冬酶-8介导的死亡受体途径导致凋亡。此外,数据表明UCLA1通过直接结合HIV-1和间接防止MDM感染来保护心肌细胞免受半胱天冬酶介导的凋亡。